

Impact of COPD diagnosis timing on clinical and economic outcomes: the ARCTIC observational cohort study
- PMID: 31190785
- PMCID: PMC6526023
- DOI: 10.2147/COPD.S195382
Impact of COPD diagnosis timing on clinical and economic outcomes: the ARCTIC observational cohort study
Abstract
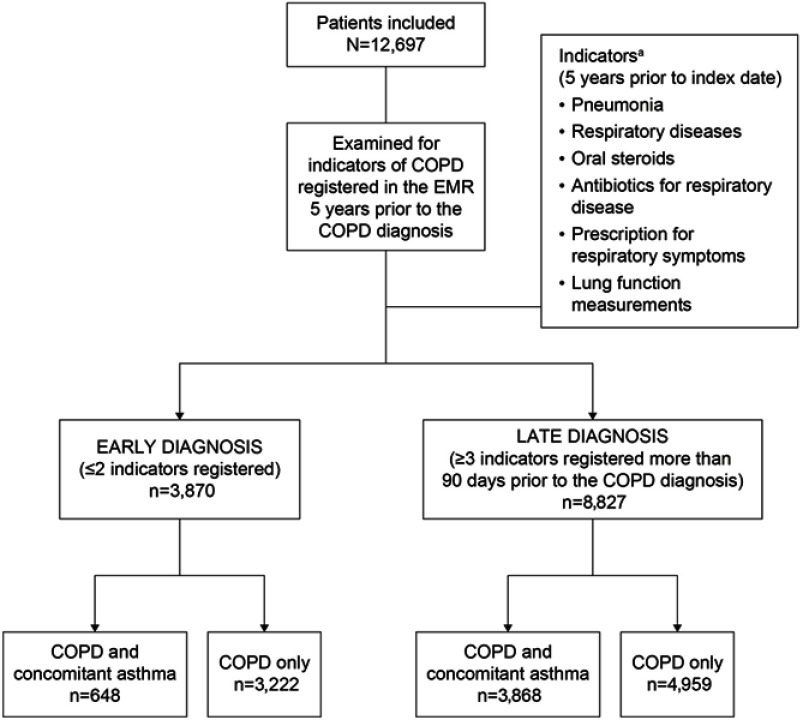
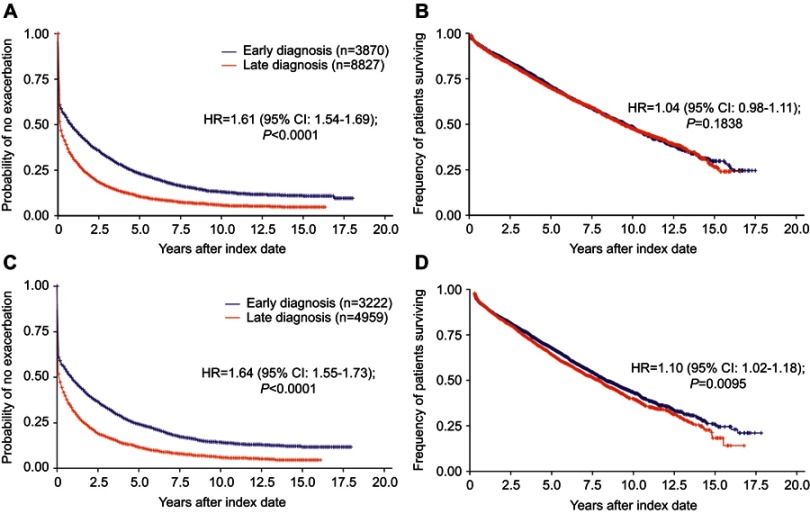
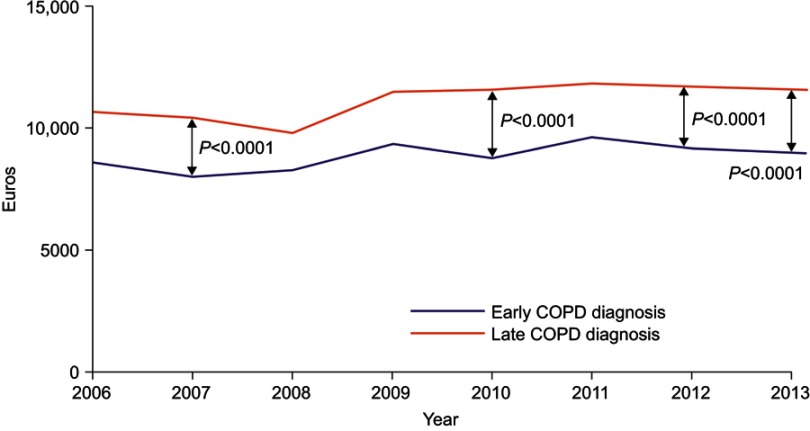
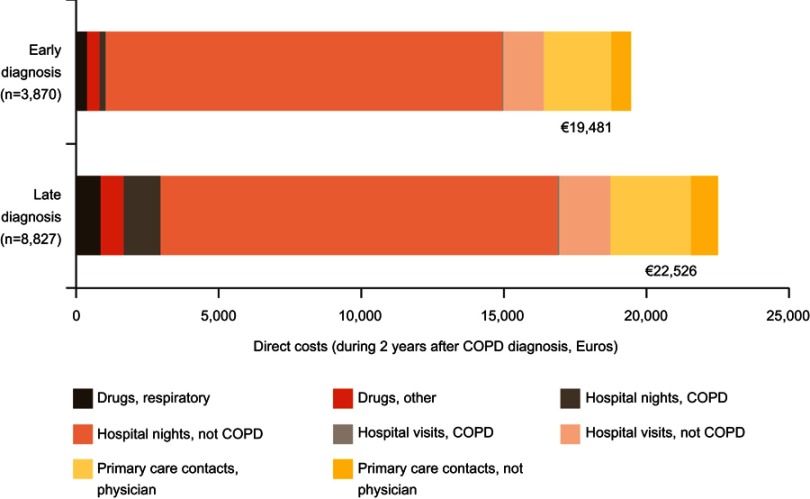
Purpose: Assess the clinical and economic consequences associated with an early versus late diagnosis in patients with COPD. Patients and methods: In a retrospective, observational cohort study, electronic medical record data (2000-2014) were collected from Swedish primary care patients with COPD. COPD indicators (pneumonia, other respiratory diseases, oral corticosteroids, antibiotics for respiratory infections, prescribed drugs for respiratory symptoms, lung function measurement) registered prior to diagnosis were applied to categorize patients into those receiving early (2 or less indicators) or late diagnosis (3 or more indicators registered >90 days preceding a COPD diagnosis). Outcome measures included annual rate of and time to first exacerbation, mortality risk, prevalence of comorbidities and health care utilization. Results: More patients with late diagnosis (n=8827) than with early diagnosis (n=3870) had a recent comorbid diagnosis of asthma (22.0% vs 3.9%; P<0.0001). Compared with early diagnosis, patients with late diagnosis had a higher exacerbation rate (hazard ratio [HR] 1.89, 95% confidence interval [CI]: 1.83-1.96; P<0.0001) and shorter time to first exacerbation (HR 1.61, 95% CI: 1.54-1.69; P<0.0001). Mortality was not different between groups overall but higher for late versus early diagnosis, after excluding patients with past asthma diagnosis (HR 1.10, 95% CI: 1.02-1.18; P=0.0095). Late diagnosis was also associated with higher direct costs than early diagnosis. Conclusion: Late COPD diagnosis is associated with higher exacerbation rate and increased comorbidities and costs compared with early diagnosis. The study highlights the need for accurate diagnosis of COPD in primary care in order to reduce exacerbations and the economic burden of COPD.
Keywords: Sweden; chronic obstructive pulmonary disease; diagnosis; exacerbations; mortality.
Conflict of interest statement
KjL has, during the last 5 years, on one or more occasion served in an advisory board and/or served as speaker and/or participated in education arranged by AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Orion, Takeda, Novartis, Chiesi and TEVA. CJ has received honoraria for educational activities and lectures from AstraZeneca, Boehringer Ingelheim, Chiesi, Novartis and TEVA, and has served on advisory boards arranged by AstraZeneca, TEVA and Boehringer Ingelheim. BS has received honoraria for educational activities and lectures from AstraZeneca, Boehringer Ingelheim, GlaxoSmithKline, Novartis, MEDA and TEVA, and has served on advisory boards arranged by AstraZeneca, Novartis, GlaxoSmithKline and Boehringer Ingelheim. KL has participated in the steering committee by Novartis for this study and received honoraria for educational activities and lectures from AstraZeneca, GlaxoSmithKline, Novartis, MEDA and TEVA and has served on advisory boards arranged by MEDA and Novartis. FSG and JBG are employees of Novartis Pharma AG. PO is an employee of Novartis AB. MU and LJ are employees of IQVIA, who received remuneration in relation to statistical analysis. GJ has participated in the steering committee by Novartis for this study and served on advisory boards arranged by AstraZeneca, Novo Nordisk and Takeda. BS reports personal fees from Novartis, during the conduct of the study; received personal fees from AstraZeneca, Novartis, Meda, Teva, Boehringer Ingelheim, and GlaxosSmithKline, outside the submitted work; KL reports personal fees from Novartis, during the conduct of the study; received personal fees from AstraZeneca, Novartis, Chiesi, TEVA, GlaxoSmithKline, and Boerhringer Ingelheim, outside the submitted work; KK was an employee of Novartis, the sponsor of the study, at the time of conduct of this analysis and until 31.10.2018. He is now affiliated with Respiratory Medicine Department, University of Ioannina, Ioannina, Greece. KK has received honoraria for educational activities and lectures from AstraZeneca, Boehringer Ingelheim, Chiesi, ELPEN, GlaxoSmithKline, MSD, Novartis, Takeda, and UCB, and has served on advisory boards arranged by AstraZeneca, Chiesi, ELPEN, Novartis and Takeda prior to 2015. The authors report no other conflicts of interest in this work.
Figures
References
-
- Global Initiative for Chronic Obstructive Lung Disease (GOLD) [webpage from Internet]. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2018. Available from: http://goldcopd.org/gold-reports/. Accessed November28, 2018.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
