

Plasma indoleamine 2,3-dioxygenase activity as a potential biomarker for early diagnosis of multidrug-resistant tuberculosis in tuberculosis patients
- PMID: 31190914
- PMCID: PMC6526328
- DOI: 10.2147/IDR.S202369
Plasma indoleamine 2,3-dioxygenase activity as a potential biomarker for early diagnosis of multidrug-resistant tuberculosis in tuberculosis patients
Abstract
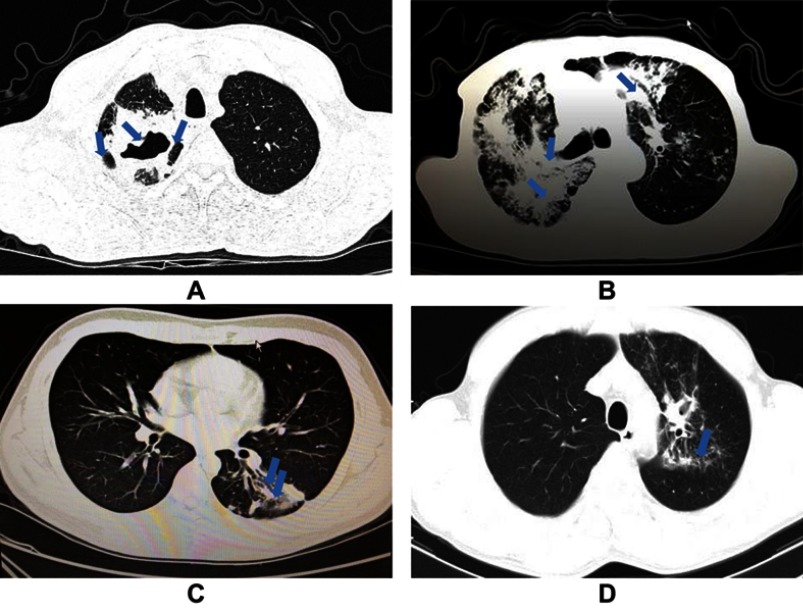
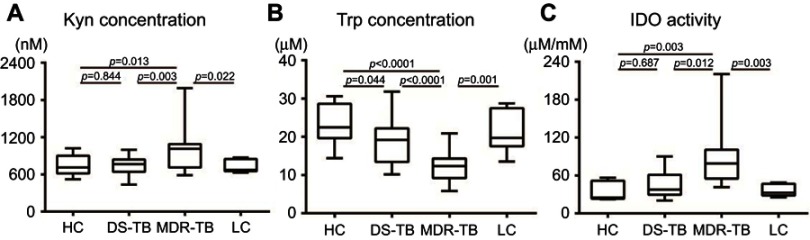
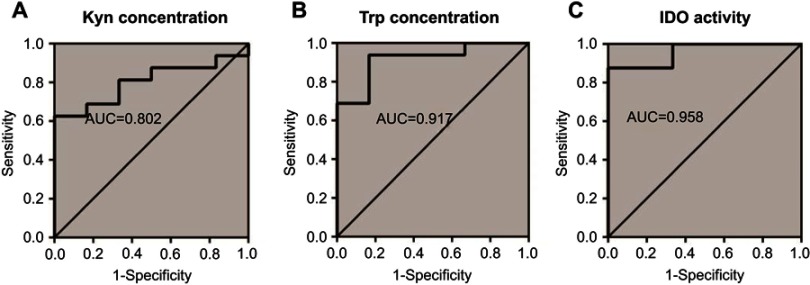
Purpose: Multidrug-resistant tuberculosis (MDR-TB) remains a challenge of global TB control, with difficulty in early detection of drug-sensitive tuberculosis (DS-TB). We investigate the diagnostic significance of IDO as a potential biomarker to discriminate MDR patients among the TB patients. Patients and methods: Plasma indoleamine 2,3-dioxygenase (IDO) was measured by the ratio of kynurenine (Kyn) to tryptophan (Trp) concentrations, using high performance liquid chromatography-mass spectrometry (LC-MS/MS). Chest computed tomography (CT) imaging signs from TB patients were collected and analyzed in 18 DS-TB patients, 16 MDR-TB patients, 6 lung cancer (LC) patients, and 11 healthy individuals. Lung imaging signs from TB patients were collected and analyzed. Results: We found that plasma IDO activity was significantly higher in the MDR-TB patients than in the DS-TB patients (p=0.012) and in the LC patients (p=0.003). We evaluated the diagnostic significance of plasma IDO activity in discriminating the MDR-TB group from the DS-TB group using a receiver operating characteristic (ROC) curve. With a cutoff level of 46.58 uM/mM, the diagnostic sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for IDO activity were 87.50%, 72.22%, 73.68%, and 86.67%, respectively. Plasma IDO activity was higher in cavity cases than in non-cavity cases (p=0.042), proving a positive correlation between lung cavity number and cavity size (p<0.05, separately) among all the TB patients studied. Conclusion: Our findings confirmed that plasma IDO activity might have an auxiliary diagnosis value for early discrimination of MDR-TB patients from DS-TB patients. Among the TB patients with cavitary lung lesions, higher plasma IDO activity can indicate a higher risk of MDR-TB.
Keywords: IDO; LC-MS/MS; MDR-TB; cavitary lung lesion.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures


Similar articles
-
Indoleamine 2, 3-Dioxygenase-Mediated Tryptophan Catabolism: A Leading Star or Supporting Act in the Tuberculosis and HIV Pas-de-Deux?Front Cell Infect Microbiol. 2019 Oct 29;9:372. doi: 10.3389/fcimb.2019.00372. eCollection 2019. Front Cell Infect Microbiol. 2019. PMID: 31737575 Free PMC article. Review.
-
Serum indoleamine 2,3-dioxygenase activity predicts prognosis of pulmonary tuberculosis.Clin Vaccine Immunol. 2012 Mar;19(3):436-42. doi: 10.1128/CVI.05402-11. Epub 2012 Jan 4. Clin Vaccine Immunol. 2012. PMID: 22219312 Free PMC article.
-
Plasma Indoleamine 2, 3-Dioxygenase, a Biomarker for Tuberculosis in Human Immunodeficiency Virus-Infected Patients.Clin Infect Dis. 2017 Oct 15;65(8):1356-1358. doi: 10.1093/cid/cix550. Clin Infect Dis. 2017. PMID: 29017244 Free PMC article.
-
Diagnostic accuracy of plasma kynurenine/tryptophan ratio, measured by enzyme-linked immunosorbent assay, for pulmonary tuberculosis.Int J Infect Dis. 2020 Oct;99:441-448. doi: 10.1016/j.ijid.2020.08.028. Epub 2020 Aug 12. Int J Infect Dis. 2020. PMID: 32800860
-
Tryptophan and Its Derived Metabolites as Biomarkers for Tuberculosis Disease: A Systematic Review.Iran Biomed J. 2024 Jul 1;28(4):140-7. doi: 10.61186/ibj.4174. Iran Biomed J. 2024. PMID: 39034495 Free PMC article.
Cited by
-
Indoleamine 2, 3-Dioxygenase-Mediated Tryptophan Catabolism: A Leading Star or Supporting Act in the Tuberculosis and HIV Pas-de-Deux?Front Cell Infect Microbiol. 2019 Oct 29;9:372. doi: 10.3389/fcimb.2019.00372. eCollection 2019. Front Cell Infect Microbiol. 2019. PMID: 31737575 Free PMC article. Review.
-
Normative Data on Serum and Plasma Tryptophan and Kynurenine Concentrations from 8089 Individuals Across 120 Studies: A Systematic Review and Meta-Analysis.Int J Tryptophan Res. 2023 Nov 29;16:11786469231211184. doi: 10.1177/11786469231211184. eCollection 2023. Int J Tryptophan Res. 2023. PMID: 38034059 Free PMC article.
-
Understanding Metabolic Regulation Between Host and Pathogens: New Opportunities for the Development of Improved Therapeutic Strategies Against Mycobacterium tuberculosis Infection.Front Cell Infect Microbiol. 2021 Mar 16;11:635335. doi: 10.3389/fcimb.2021.635335. eCollection 2021. Front Cell Infect Microbiol. 2021. PMID: 33796480 Free PMC article. Review.
-
The Kynurenine/Tryptophan Ratio as a Promising Metabolomic Biomarker for Diagnosing the Spectrum of Tuberculosis Infection and Disease.Int J Gen Med. 2023 Nov 28;16:5587-5595. doi: 10.2147/IJGM.S438364. eCollection 2023. Int J Gen Med. 2023. PMID: 38045904 Free PMC article. Review.
-
Chinese expert consensus on imaging diagnosis of drug-resistant pulmonary tuberculosis.Quant Imaging Med Surg. 2024 Jan 3;14(1):1039-1060. doi: 10.21037/qims-23-1223. Epub 2023 Oct 25. Quant Imaging Med Surg. 2024. PMID: 38223121 Free PMC article. Review.
References
-
- World Health Organization. Global tuberculosis report 2018, Geneva: https://www.who.int/tb/publications/global_report/en/. Accessed September 18, 2018.
-
- World Health Organization (Producer). Use of high burden country lists for TB by WHO in the post-2015 era, June 2015 meeting of WHO’s Strategic and technical advisory group for TB (STAG-TB). WHO/HTM/TB/2015.29. Geneva: World Health Organization; 2015
LinkOut - more resources
Full Text Sources
Research Materials
