

Multiple Sclerosis at Home Access (MAHA): An Initiative to Improve Care in the Community
- PMID: 31191175
- PMCID: PMC6552994
- DOI: 10.7224/1537-2073.2018-006
Multiple Sclerosis at Home Access (MAHA): An Initiative to Improve Care in the Community
Abstract
Background: Caring for individuals with progressive, disabling forms of multiple sclerosis (MS) presents ongoing, complex challenges in health care delivery, especially access to care. Although mobility limitations represent a major hurdle to accessing comprehensive and coordinated care, fragmentation in current models of health care delivery magnify the problem. Importantly, individuals with disabling forms of MS are exceedingly likely to develop preventable secondary complications and to incur significant suffering and increased health care utilization and costs.
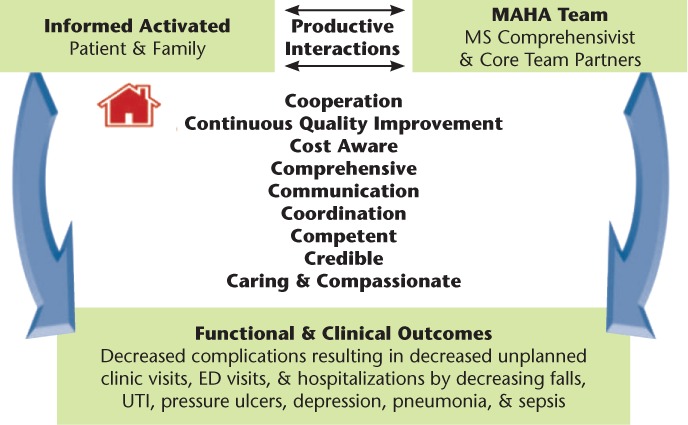
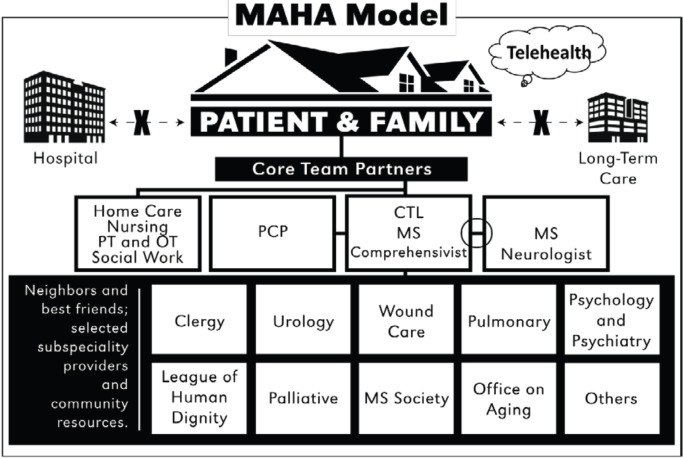
Methods: A house call program, Multiple Sclerosis at Home Access (MAHA), was implemented. The program was designed to provide comprehensive services and prevent common complications. Key aspects included monthly house calls, continuity among providers, and a multidisciplinary team led by a comprehensivist, a provider bridging subspecialty and primary care. A total of 21 adult patients (Expanded Disability Status Scale score ≥7.5) completed 1 full year of the program.
Results: During the 2-year preevaluation and postevaluation period, half of the hospital admissions were related to secondary and generally preventable complications. Aside from a single outlying individual important to the evaluation, in the year after program implementation, decreases were found in number of individuals hospitalized, hospitalizations/skilled facility admissions, and hospital days; the total number of overall emergency department (ED) visits decreased; and ED-only visits increased (ie, ED visits without hospital admission). Patient satisfaction reports and quality indicators were positive. Fifty percent of patients participated in supplementary televisits.
Conclusions: This program evaluation suggests that a house call-based practice is a viable solution for improving care delivery for patients with advanced MS and disability.
Keywords: Comprehensive care; Disability; House call; Multidisciplinary team; Multiple sclerosis (MS); Progressive multiple sclerosis; Telemedicine.
Conflict of interest statement
Dr. Healey has received grants from the Multiple Sclerosis Foundation. Dr. Zabad has been a site investigator or principal investigator for clinical trials funded by Biogen, Genentech, Novartis, and Sun Pharma; in the past 2 years, has served as a consultant for Bayer, Genzyme, Teva Neuroscience, and TG Therapeutics and has given unbranded lectures sponsored by Teva; and is also a member of the adjudication committee for a clinical trial of biotin in primary and secondary progressive MS sponsored by PAREXEL and MedDay Pharmaceuticals. The other authors declare no conflicts of interest.
Figures
Similar articles
-
A home-based comprehensive care model in patients with Multiple Sclerosis: A study pre-protocol.F1000Res. 2015 Sep 18;4:872. doi: 10.12688/f1000research.7040.1. eCollection 2015. F1000Res. 2015. PMID: 26673815 Free PMC article.
-
Community-based care for the specialized management of heart failure: an evidence-based analysis.Ont Health Technol Assess Ser. 2009;9(17):1-42. Epub 2009 Nov 1. Ont Health Technol Assess Ser. 2009. PMID: 23074521 Free PMC article.
-
The impact of knowledge on attitudes of emergency department staff towards patients with substance related presentations: a quantitative systematic review protocol.JBI Database System Rev Implement Rep. 2015 Oct;13(10):133-45. doi: 10.11124/jbisrir-2015-2203. JBI Database System Rev Implement Rep. 2015. PMID: 26571289
-
Mitoxantrone: a review of its use in multiple sclerosis.CNS Drugs. 2004;18(6):379-96. doi: 10.2165/00023210-200418060-00010. CNS Drugs. 2004. PMID: 15089110 Review.
-
Temporal Trends and Predictors of Thirty-Day Readmissions and Emergency Department Visits Following Total Knee Arthroplasty in Ontario Between 2003 and 2016.J Arthroplasty. 2020 Feb;35(2):364-370. doi: 10.1016/j.arth.2019.09.015. Epub 2019 Sep 14. J Arthroplasty. 2020. PMID: 31732370 Review.
Cited by
-
Electronic Health Interventions in the Case of Multiple Sclerosis: From Theory to Practice.Brain Sci. 2021 Feb 2;11(2):180. doi: 10.3390/brainsci11020180. Brain Sci. 2021. PMID: 33540640 Free PMC article. Review.
-
The reliability and validity of the Turkish version of the Telemedicine Satisfaction and Usefulness Questionnaire (TSUQ) and Telemedicine Patient Questionnaire (TPQ) in individuals with multiple sclerosis.Neurol Sci. 2022 Mar;43(3):1921-1927. doi: 10.1007/s10072-021-05519-1. Epub 2021 Aug 3. Neurol Sci. 2022. PMID: 34342782 Free PMC article.
-
Telemedicine during the Coronavirus Disease (COVID-19) Pandemic: A Multiple Sclerosis (MS) Outpatients Service Perspective.Neurol Int. 2021 Jan 18;13(1):25-31. doi: 10.3390/neurolint13010003. Neurol Int. 2021. PMID: 33477432 Free PMC article.
-
Person-centred integrated care for people living with Parkinson's, Huntington's and Multiple Sclerosis: A systematic review.Health Expect. 2024 Feb;27(1):e13948. doi: 10.1111/hex.13948. Health Expect. 2024. PMID: 39102669 Free PMC article.
References
-
- Minden SL, Frankel D, Hadden L, Perloffp J, Srinath KP, Hoaglin DC. The Sonya Slifka Longitudinal Multiple Sclerosis Study: methods and sample characteristics. Mult Scler. 2006;12:24–38. - PubMed
-
- Wallin MT. The prevalence of multiple sclerosis in the United States: a population-based healthcare database approach. ECTRIMS Online Library. Oct 26, 2017. Abstract P344.
-
- Foley PL, Vesterinen HM, Laird BJ et al. Prevalence and natural history of pain in adults with multiple sclerosis: systematic review and meta-analysis. Pain. 2013;154:632–642. - PubMed
-
- Naci H, Fleurence R, Birt J, Duhig A. The impact of increasing neurological disability of multiple sclerosis on health utilities: a systematic review of the literature. J Med Econ. 2010;13:78–89. - PubMed
-
- National Multiple Sclerosis Society Strategic Response White Paper 2011–2015. New York, NY: National Multiple Sclerosis Society; 2016.
LinkOut - more resources
Full Text Sources
Miscellaneous