

How to prepare and manage a systematic review and meta-analysis of clinical studies
- PMID: 31191989
- PMCID: PMC6540947
- DOI: 10.1302/2058-5241.4.180049
How to prepare and manage a systematic review and meta-analysis of clinical studies
Abstract
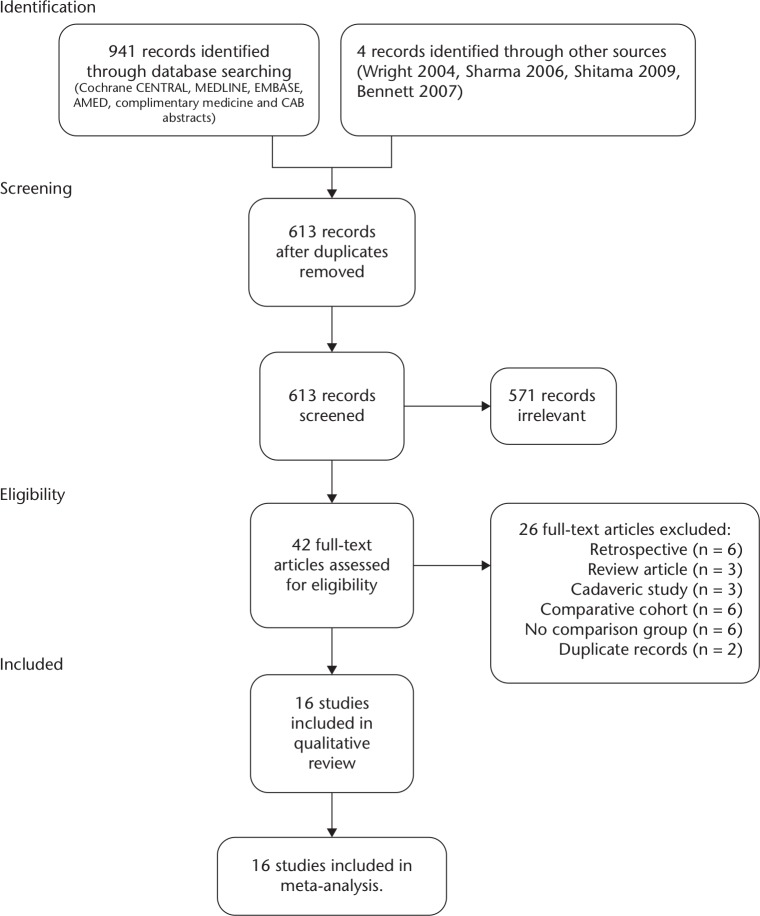
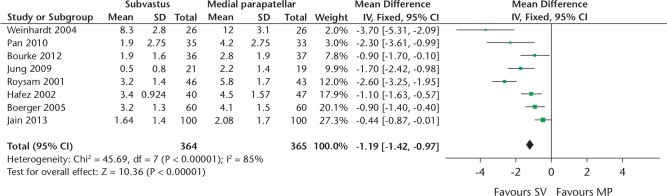
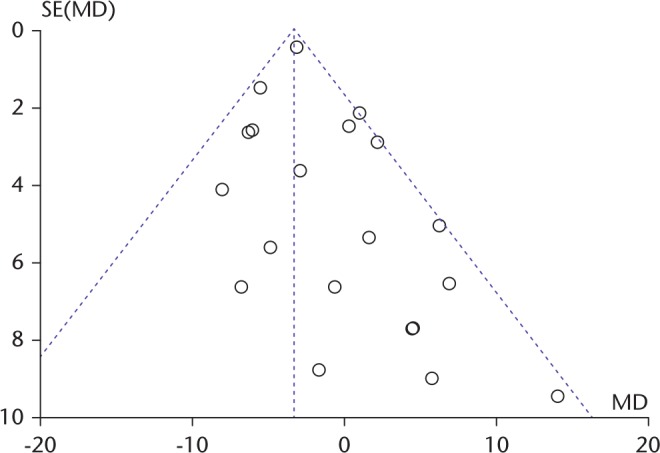
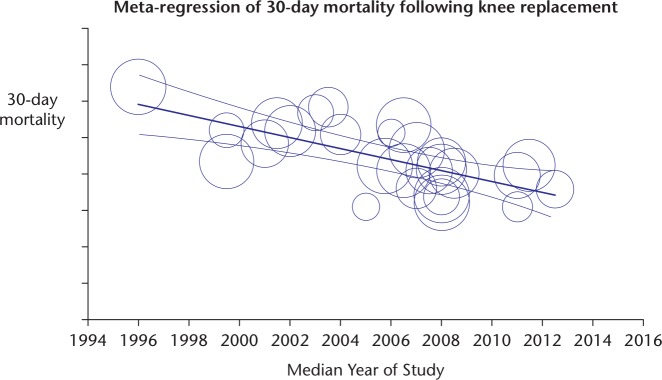
Use the PICO framework to formulate a specific clinical question.Formulate a search strategy.Prospectively register the review protocol.Execute the literature search.Apply eligibility criteria to exclude irrelevant studies.Extract data and appraise each study for risk of bias and external validity.Provide a narrative review.If appropriate data are available, perform a meta-analysis.Report the review findings in the context of the risk of bias assessment, any sensitivity analyses and the analysis of risk of publication bias.Useful resources include the Cochrane Handbook, PROSPERO, GRADE and PRISMA. Cite this article: EFORT Open Rev 2019;4:213-220. DOI: 10.1302/2058-5241.4.180049.
Keywords: meta-analysis; orthopaedics; review; systematic review.
Conflict of interest statement
ICMJE Conflict of interest statement: JRB reports that he works for North Bristol NHS trust as an Orthopaedic Surgeon and is not employed elsewhere. MRW reports that he has received a grant from National Institute for Health Research (NIHR) and that this study was supported by the NIHR Biomedical Research Centre at University Hospitals Bristol NHS Foundation Trust and the University of Bristol. The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care. He reports he has received a grant from Stryker investigate the outcome of the Triathlon total knee replacement. He has received payment for lectures including service on speakers’ bureaus from Heraeus, DePuy and that his institution receives payment at market rates for teaching on basic science and cemented joint replacement delivered to trainees and consultants.
Figures

Similar articles
-
Evaluating characteristics of PROSPERO records as predictors of eventual publication of non-Cochrane systematic reviews: a meta-epidemiological study protocol.Syst Rev. 2018 Mar 9;7(1):43. doi: 10.1186/s13643-018-0709-6. Syst Rev. 2018. PMID: 29523200 Free PMC article.
-
Clinical, behavioural and pharmacogenomic factors influencing the response to levothyroxine therapy in patients with primary hypothyroidism-protocol for a systematic review.Syst Rev. 2017 Mar 21;6(1):60. doi: 10.1186/s13643-017-0457-z. Syst Rev. 2017. PMID: 28327186 Free PMC article.
-
Use of Apps to Promote Childhood Vaccination: Protocol for a Systematic Review.JMIR Res Protoc. 2020 Feb 5;9(2):e16929. doi: 10.2196/16929. JMIR Res Protoc. 2020. PMID: 32022694 Free PMC article.
-
Human epidemiological evidence about the associations between exposure to organochlorine chemicals and endometriosis: Systematic review and meta-analysis.Environ Int. 2019 Feb;123:209-223. doi: 10.1016/j.envint.2018.11.065. Epub 2018 Dec 6. Environ Int. 2019. PMID: 30530163
-
Comparison of external and internal implant-abutment connections for implant supported prostheses. A systematic review and meta-analysis.J Dent. 2018 Mar;70:14-22. doi: 10.1016/j.jdent.2017.12.001. Epub 2017 Dec 6. J Dent. 2018. PMID: 29221955
Cited by
-
Melatonin improves fertilization rate in assisted reproduction: Systematic review and meta-analysis.Clinics (Sao Paulo). 2024 Jul 5;79:100397. doi: 10.1016/j.clinsp.2024.100397. eCollection 2024. Clinics (Sao Paulo). 2024. PMID: 38971124 Free PMC article.
-
Conducting publishable research under conditions of severely limited resources.Libyan J Med. 2020 Dec;15(1):1688126. doi: 10.1080/19932820.2019.1688126. Libyan J Med. 2020. PMID: 31680657 Free PMC article.
-
Chronic endometritis and assisted reproduction: a systematic review and meta-analysis.Rev Assoc Med Bras (1992). 2023 Oct 13;69(10):e20230792. doi: 10.1590/1806-9282.20230792. eCollection 2023. Rev Assoc Med Bras (1992). 2023. PMID: 37851720 Free PMC article. No abstract available.
-
Previous preeclampsia and its association with the future development of cardiovascular diseases: a systematic review and meta-analysis.Clinics (Sao Paulo). 2021 Jan 20;76:e1999. doi: 10.6061/clinics/2021/e1999. eCollection 2021. Clinics (Sao Paulo). 2021. PMID: 33503177 Free PMC article.
-
Exercise training and experimental myocardial ischemia and reperfusion: A systematic review and meta-analysis.Int J Cardiol Heart Vasc. 2023 Apr 29;46:101214. doi: 10.1016/j.ijcha.2023.101214. eCollection 2023 Jun. Int J Cardiol Heart Vasc. 2023. PMID: 37181278 Free PMC article. Review.
References
-
- Moseley JB, O’Malley K, Petersen NJ, et al. A controlled trial of arthroscopic surgery for osteoarthritis of the knee. N Engl J Med 2002;347(2):81–88. - PubMed
-
- Lind J. A Treatise of the Scurvy. In three parts. Containing an inquiry into the nature, causes, and cure, of that disease, etc: Edinburgh; 1753.
-
- Chalmers I, Altman DG. Systematic reviews. London: BMJ Publishing Group, 1995.
Publication types
LinkOut - more resources
Full Text Sources
