

Tectonic Keratoplasty to Restore the Bulbar Wall after Block Excision of Benign and Malignant Intraocular Tumors
- PMID: 31191996
- PMCID: PMC6525849
- DOI: 10.1155/2019/4153064
Tectonic Keratoplasty to Restore the Bulbar Wall after Block Excision of Benign and Malignant Intraocular Tumors
Abstract
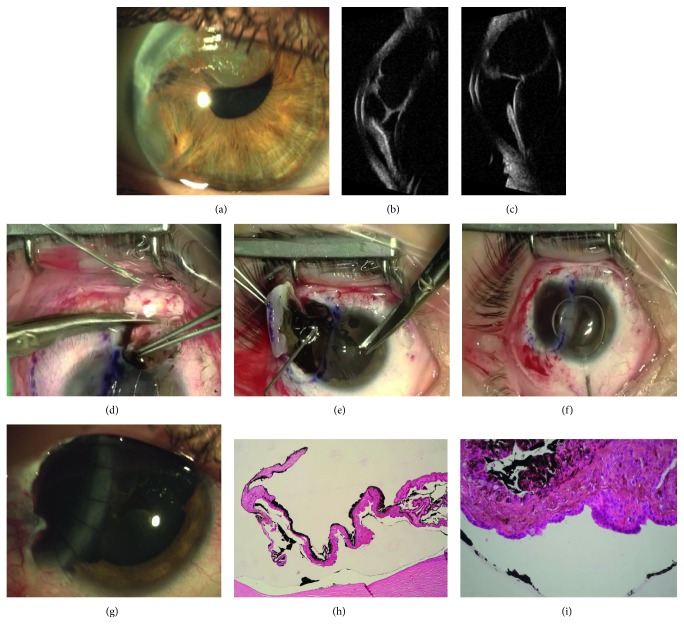
Purpose: To report the surgical treatment and follow-up of tumors of the anterior uvea and epithelial cysts of the anterior chamber in 4 patients submitted to block excision and tectonic corneal graft between 2008 and 2012.
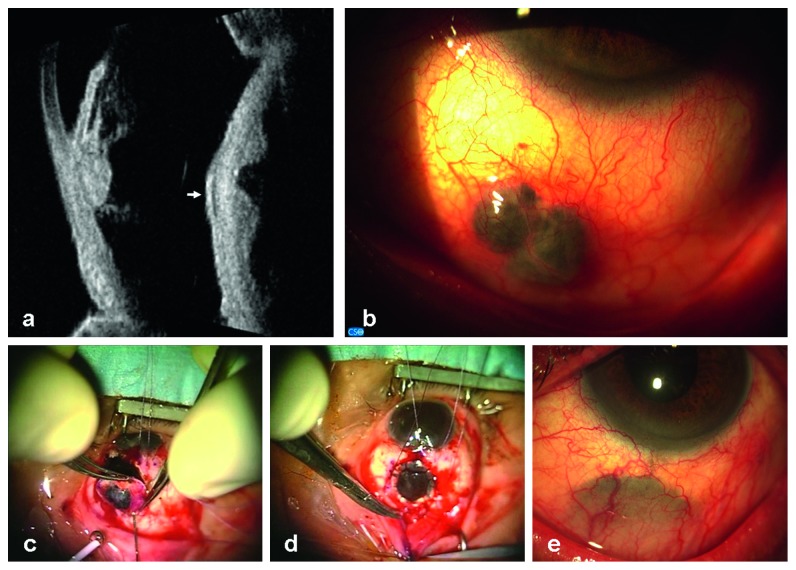
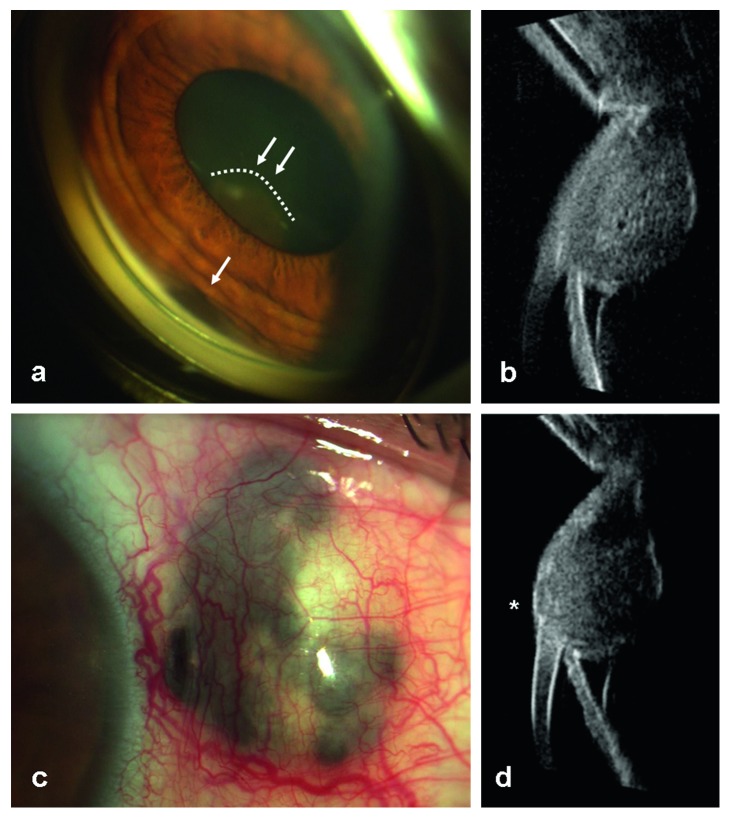
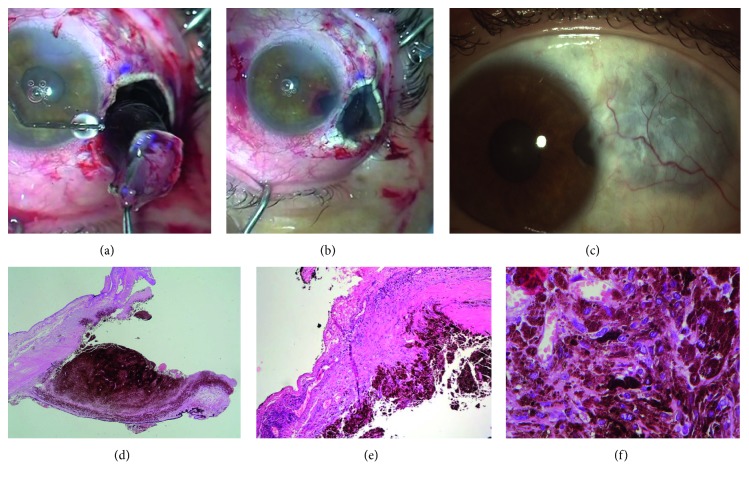
Methods: This is a retrospective, nonrandomized case series. Two patients were affected by anterior uveal malignant melanoma, and 2 patients were referred to us for large epithelial iris cysts with anterior chamber angle involvement and partial corneal failure. A simultaneous block removal of the lesion and adjacent iris, cornea (when necessary), ciliary body, and sclera was performed; the resulting defect was covered by a tectonic whole thickness corneal graft. Follow-up ranged from 2 to 7 years (mean time: 5 ± 1.6 MD).
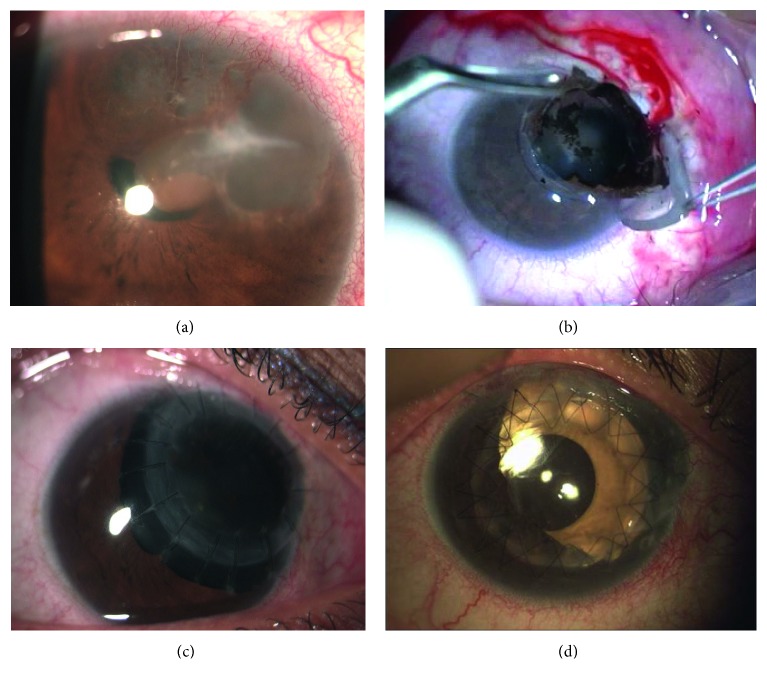
Results: Local control of malignant melanoma was observed during the follow-up, but cataract surgery was planned in both patients and pars plana vitrectomy for vitreous hemorrhage occurred in one case. No recurrence of cysts was detected. After iris cysts excision, a planned second-time surgery was necessary in one patient: optical penetrating keratoplasty, centered on the visual axis, implantation of one refractive IOL (intraocular lens) in the bag, and one cosmetic IOL in the sulcus, to restore the iris diaphragm.
Conclusions: Block excision followed by the tectonic corneal graft seems to be the treatment of choice for selected cases of epithelial cysts of the anterior chamber and anterior uvea melanomas with epibulbar extension. Further surgery, as a second step, could be required to improve functional results of this challenging technique.
Figures
Similar articles
-
Block excision of tumors of the anterior uvea. Report on 68 consecutive patients.Ophthalmology. 1996 Dec;103(12):2017-27; discussion 2027-8. doi: 10.1016/s0161-6420(96)30392-8. Ophthalmology. 1996. PMID: 9003335
-
[Block excision with tectonic corneoscleroplasty for cystic and/or diffuse epithelial invasion of the anterior eye segment. Report of 51 consecutive patients (1980-1996)].Klin Monbl Augenheilkd. 1997 Nov;211(5):312-23. doi: 10.1055/s-2008-1035141. Klin Monbl Augenheilkd. 1997. PMID: 9527589 German.
-
Rhegmatogenous retinal detachment after block excision of epithelial implantation cysts and tumors of the anterior uvea.Ophthalmology. 1999 Oct;106(10):1942-6. doi: 10.1016/S0161-6420(99)90405-0. Ophthalmology. 1999. PMID: 10519589
-
[Intraocular lens explantation and retroiridal iris claw lens implantation via the pars plana : Video article].Ophthalmologe. 2020 Nov;117(11):1133-1137. doi: 10.1007/s00347-020-01246-8. Ophthalmologe. 2020. PMID: 33034738 Review. German.
-
[Sutureless scleral intraocular lens fixation: report of nine cases and literature review].J Fr Ophtalmol. 2013 Oct;36(8):658-68. doi: 10.1016/j.jfo.2012.09.009. Epub 2013 Jul 25. J Fr Ophtalmol. 2013. PMID: 23891322 Review. French.
References
-
- Zirm E. Über endobulbäre operation. Arch Augenheilkd. 1911;69:233–236.
LinkOut - more resources
Full Text Sources
Miscellaneous
