

Cytokines and the Pathogenesis of Macular Edema in Branch Retinal Vein Occlusion
- PMID: 31191997
- PMCID: PMC6525954
- DOI: 10.1155/2019/5185128
Cytokines and the Pathogenesis of Macular Edema in Branch Retinal Vein Occlusion
Abstract
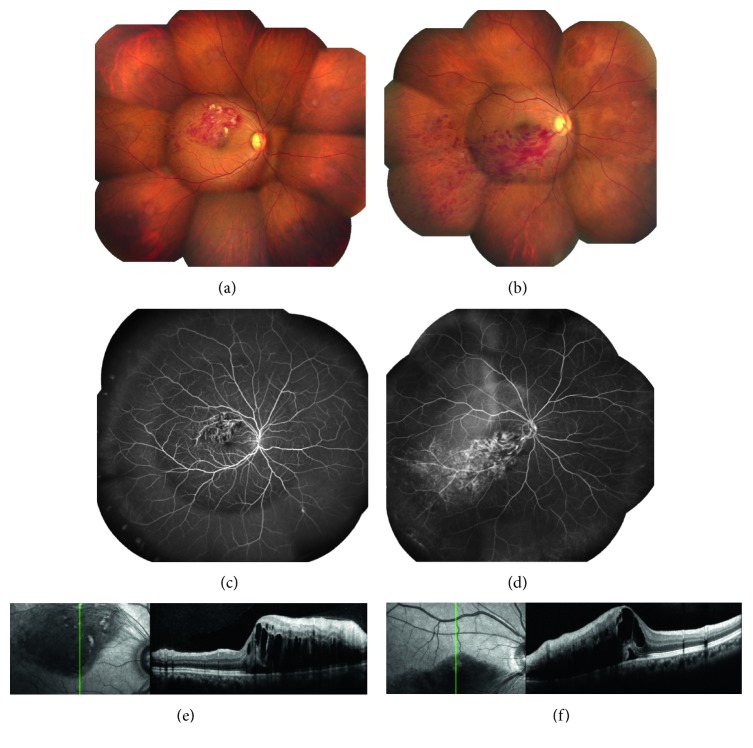
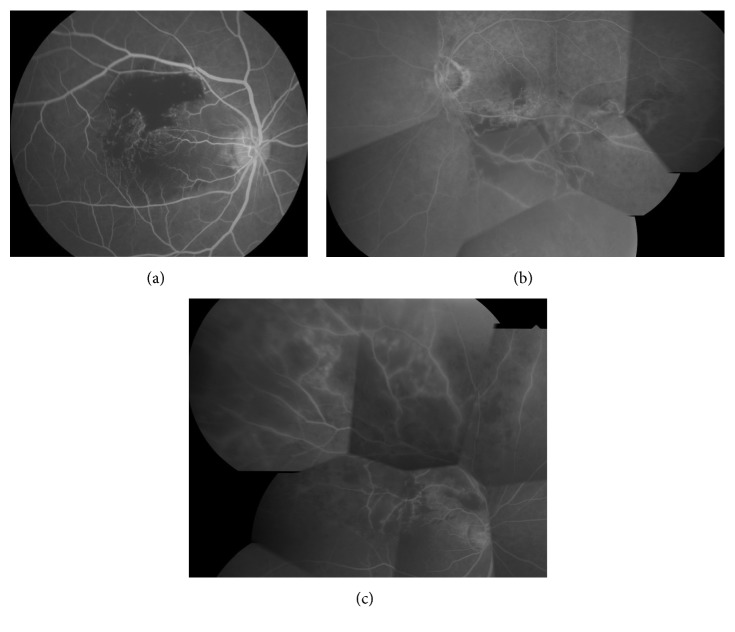
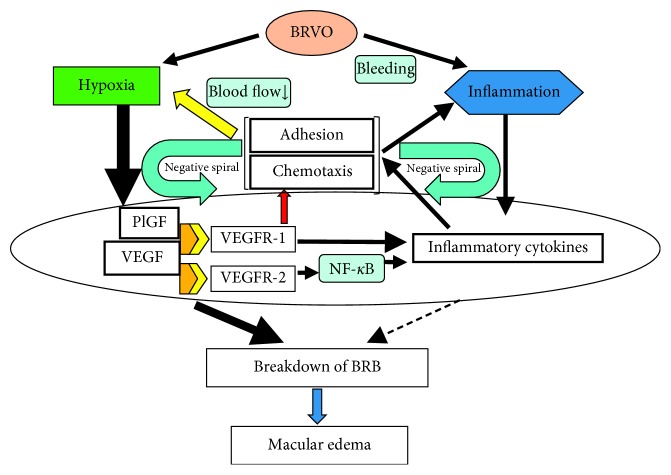
Branch retinal vein occlusion (BRVO) is a very common retinal vascular problem in patients with lifestyle-related diseases, such as hypertension and arteriosclerosis. In patients with BRVO, development of macular edema is the main cause of visual impairment. BRVO is still a controversial condition in many respects. Over the years, various methods such as laser photocoagulation have been tried to treat macular edema associated with BRVO, but the results were not satisfactory. After vascular endothelial growth factor (VEGF) was found to have an important role in the pathogenesis of macular edema in BRVO patients, treatment of this condition was revolutionized by development of anti-VEGF therapy. Although macular edema improves dramatically following intraocular injection of anti-VEGF agents, repeated recurrence and resistance of edema is a major problem in some BRVO patients. This suggests that factors or cytokines other than VEGF may be associated with inflammation and retinal hypoxia in BRVO and that the pathogenesis of macular edema is complicated. The present review assesses the role of various factors and cytokines in the pathogenesis of macular edema associated with BRVO. We present a mechanism that is not only plausible but should also be useful for developing new therapeutic strategies.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
