

Temporal Trends in the Prevalence of Diabetes Decompensation (Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State) Among Adult Patients Hospitalized with Diabetes Mellitus: A Nationwide Analysis Stratified by Age, Gender, and Race
- PMID: 31192058
- PMCID: PMC6550510
- DOI: 10.7759/cureus.4353
Temporal Trends in the Prevalence of Diabetes Decompensation (Diabetic Ketoacidosis and Hyperosmolar Hyperglycemic State) Among Adult Patients Hospitalized with Diabetes Mellitus: A Nationwide Analysis Stratified by Age, Gender, and Race
Abstract
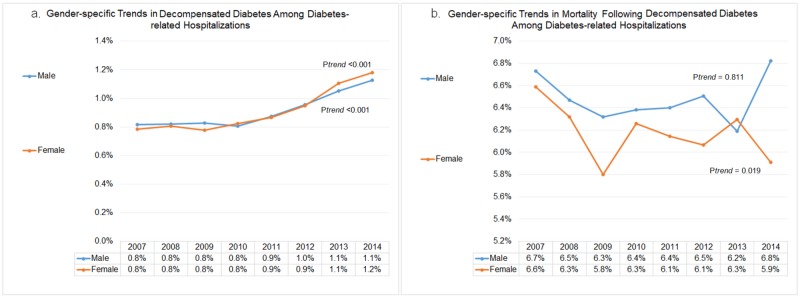
Background Disproportionate change in the burden of diabetes mellitus across various subgroups has been reported in the United States. However, changing landscape of the prevalence and mortality of decompensated diabetes (diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS)) remains indistinct across various age, gender, and racial groups of hospitalized diabetics. Methods The National Inpatient Sample (NIS) datasets (2007-2014) were sought to assess the prevalence and temporal trends in decompensated diabetes stratified by age, gender, and race and related in-hospital outcomes among the adult patients hospitalized with diabetes using International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes. Discharge weights were used to obtain national estimates. Results Of 56.7 million hospitalizations with diabetes, 0.5 (0.9%) million patients revealed decompensated diabetes from 2007 to 2014. The decompensated diabetics consisted of younger (~52 vs. 66 yrs), more often black (24.2% vs. 17.3%) and Hispanic (12.9% vs. 10.9%) patients as compared to those without decompensation (p<0.001). Younger diabetes patients demonstrated the highest prevalence of in-hospital decompensation (18-44 yrs; 3.7%) with a relative increase of 32.4% (from 3.4% to 4.5%) from 2007 to 2014 (ptrend<0.001). Older diabetics (≥65 years) with decompensation suffered the highest in-hospital mortality (12.8%). The overall rate of decompensation was similar (0.9%) among male and female diabetes patients. However, over a period of 8 years, the rates of decompensation rose to 1.1% (ptrend<0.001) in males and 1.2% (ptrend<0.001) in females, respectively. All-cause in-hospital mortality among females with decompensated diabetes declined from 6.6% in 2007 to 5.9% in 2014 (ptrend=0.019). However, there was no significant drop in in-hospital mortality among male diabetics with acute decompensation (6.7% in 2007 to 6.8% in 2014, ptrend=0.811). We observed significantly increasing trends in decompensated diabetes among all race groups between 2007 and 2014 (ptrend<0.001). The in-hospital mortality was highest among Asian or Pacific Islander (0.9%) diabetes patients with decompensation from 2007 to 2014. There was a declining trend in the inpatient mortality among Asian or Pacific Islander (ptrend=0.029) and Hispanic (ptrend<0.001) patients with decompensated diabetes, whereas other race groups did not observe any significant decline in mortality over the study period. Diabetes hospitalizations with decompensation demonstrated significantly higher in-hospital mortality (6.3% vs. 2.6%; p<0.001), average length of stay (7.7 vs. 5.4 days; p<0.001), hospital charges ($65,904 vs. $42,889, p<0.001), and more frequent transfers to short-term hospitals (3.9% vs. 2.9%; p<0.001) in comparison to those without decompensation. The rates of acute myocardial infarction (AMI) (10.4% vs. 4.8%; p<0.001), stroke (4.0% vs. 3.3%; p<0.001) and venous thromboembolism (3.5% vs. 2.6%; p<0.001) were substantially higher among diabetics with decompensation compared to those without. Conclusions There was an increasing trend in the prevalence of decompensated diabetes from 2007 to 2014, most remarkable among younger black male diabetics. The patients with decompensated diabetes suffered higher in-hospital mortality and rates of AMI, stroke and venous thromboembolism, there was no significant decline in the mortality between 2007 and 2014.
Keywords: age gender racial disparities; decompensation; diabetes mellitus; diabetic ketoacidosis; hyperosmolar hyperglycemic state; mortality; myocardial infarction; stroke; trends.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures


References
-
- Prevalence of and trends in diabetes among adults in the united states, 1988-2012. Menke A, Casagrande S, Geiss L, Cowie CC. JAMA. 2015;314:1021–1029. - PubMed
-
- Health care utilization and burden of diabetic ketoacidosis in the U.S. Over the past decade: a nationwide analysis. Desai D, Mehta D, Mathias P, Menon G, Schubart UK. Diabetes Care. 2018;41:1631–1638. - PubMed
LinkOut - more resources
Full Text Sources