

Linac-Based Radiosurgery for Patients With Brain Oligometastases From a Breast Primary, in the Trastuzumab Era-Impact of Tumor Phenotype and Prescribed SRS Dose
- PMID: 31192116
- PMCID: PMC6547789
- DOI: 10.3389/fonc.2019.00377
Linac-Based Radiosurgery for Patients With Brain Oligometastases From a Breast Primary, in the Trastuzumab Era-Impact of Tumor Phenotype and Prescribed SRS Dose
Abstract
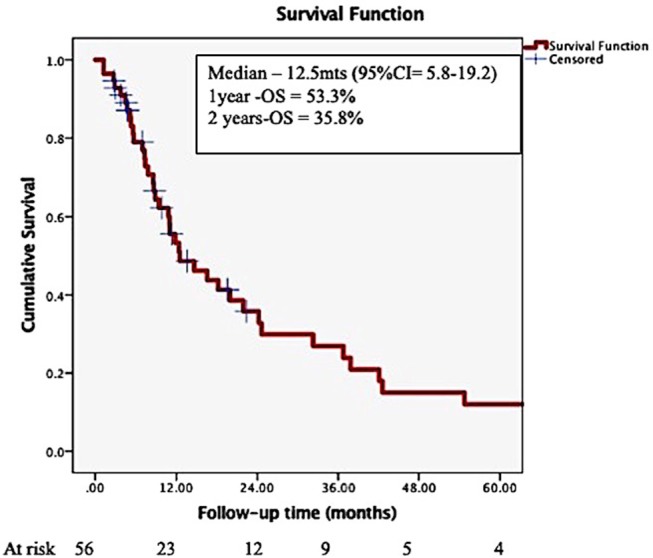
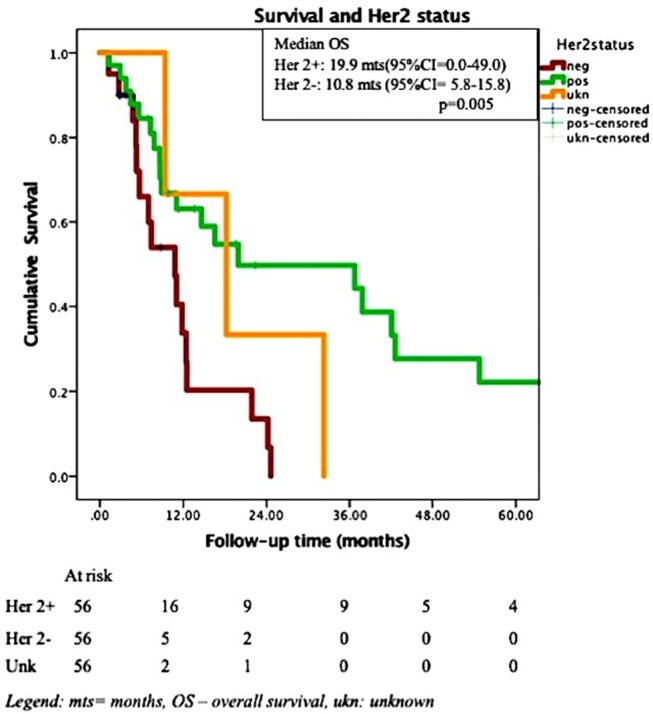
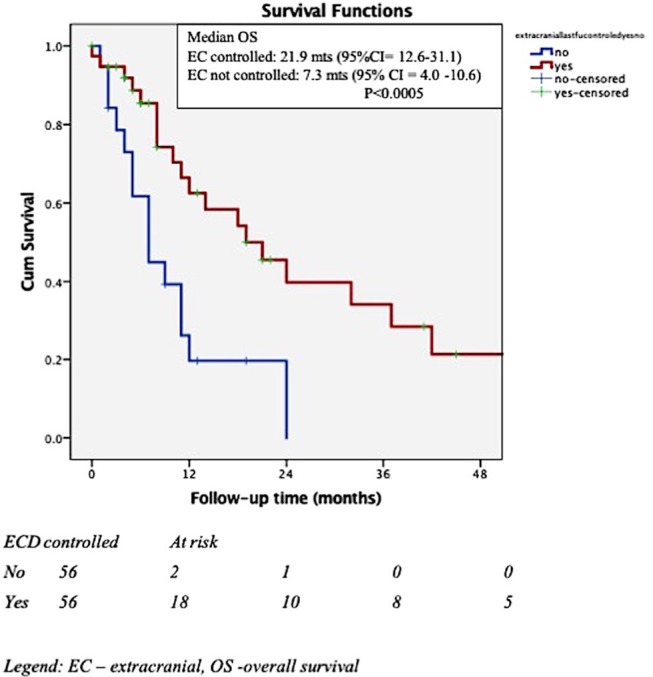
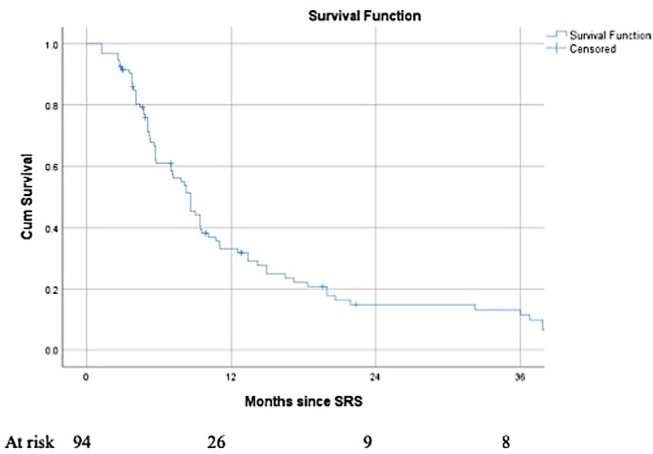
Background: The role of stereotactic radiosurgery (SRS) in the treatment of limited numbers of brain metastases in selected breast cancer patients is well-established. Aims: To analyse outcome from a single institutional experience with SRS, to identify any significant prognostic factors and to assess the influence of Her-2, estrogen receptor status, and prescribed dose on outcome. Methods: The medical records of 56 patients treated at in a single institution between 2009 and 2014 were reviewed. Demographic, treatment related and outcome data were analyzed to identify prognostic factors in this patient population. The primary endpoints were overall survival and local control. Secondary endpoint was distant intra-cranial progression-free survival. Results: The median follow- up time for the entire cohort was 10.33 months (1.25-97.28). The overall median survival was 12.5months (95%CI = 5.8-19.2), with 53.3%, and 35.8% surviving at 1- and 2- years post-SRS. After adjustment for the effect of Her 2 status, uncontrolled extra-cranial disease at the time of SRS predicted for shorter survival (HR for death = 3.1, 95% CI = 1.4-6.9, p = 0.006). At the time of death, 75% of the patients had active, uncontrolled intra-cranial disease, with 56% these patients presenting intra-cranial disease only. Sustained local control was observed in 56 (59.6%) of 94 treated metastases. In univariate analysis, Her2 status, ERHer2 group status?, and prescribed SRS dose were highly significant for local progression free-survival (LPFS). After adjustment for the effect of Her 2 status, patients receiving 12-16 Gy can expect shorter LPFS than those receiving 18-20 Gy (HR = 1.7, 95% CI = 1.0-2.8, p = 0.043). After adjustment for the effect of dose group, patients with Her 2 negative cancer can expect shorter LPFS than those with Her 2 positive cancer (HR = 2.6, 95% CI = 1.5-4.4, p < 0.0005). Use of prior WBRT did not impact survival, local or distant intra-cranial progression-free survival. Conclusions: Survival outcome is similar to the published literature. Improved outcomes are observed in patients with Her 2-positive, controlled extracranial disease at the time of SRS and higher SRS dose delivered. Achieving intra-cranial control appears to be an important factor for the survival of the breast cancer patients in the era of targeted therapies.
Keywords: Her 2 status; SRS; brain metastases; breast cancer; dose.
Figures
Similar articles
-
Potential role for LINAC-based stereotactic radiosurgery for the treatment of 5 or more radioresistant melanoma brain metastases.J Neurosurg. 2015 Nov;123(5):1261-7. doi: 10.3171/2014.12.JNS141919. Epub 2015 Jul 3. J Neurosurg. 2015. PMID: 26140482
-
Clinical outcomes of gastrointestinal brain metastases treated with radiotherapy.Radiat Oncol. 2017 Feb 28;12(1):43. doi: 10.1186/s13014-017-0774-3. Radiat Oncol. 2017. PMID: 28245881 Free PMC article.
-
Radiosurgery in the management of brain metastasis: a retrospective single-center study comparing Gamma Knife and LINAC treatment.J Neurosurg. 2018 Feb;128(2):352-361. doi: 10.3171/2016.10.JNS161480. Epub 2017 Mar 24. J Neurosurg. 2018. PMID: 28338441
-
Clinical outcomes of stereotactic radiosurgery in the treatment of patients with metastatic brain tumors.World Neurosurg. 2011 May-Jun;75(5-6):673-83. doi: 10.1016/j.wneu.2010.12.006. World Neurosurg. 2011. PMID: 21704935 Review.
-
Long-term Survival From Breast Cancer Brain Metastases in the Era of Modern Systemic Therapies.Neurosurgery. 2024 Jan 1;94(1):154-164. doi: 10.1227/neu.0000000000002640. Epub 2023 Aug 15. Neurosurgery. 2024. PMID: 37581437 Review.
Cited by
-
Validation of Nine Different Prognostic Grading Indexes for Radiosurgery of Brain Metastases in Breast Cancer Patients and Development of an All-Encompassing Prognostic Tool.Front Oncol. 2020 Sep 2;10:1557. doi: 10.3389/fonc.2020.01557. eCollection 2020. Front Oncol. 2020. PMID: 33014802 Free PMC article.
-
Stereotactic radiosurgery for patients with breast cancer brain oligometastases - molecular subtypes and clinical outcomes.Rep Pract Oncol Radiother. 2021 Feb 25;26(1):1-11. doi: 10.5603/RPOR.a2021.0001. eCollection 2021. Rep Pract Oncol Radiother. 2021. PMID: 33948296 Free PMC article.
-
Factors associated with the local control of brain metastases: a systematic search and machine learning application.BMC Med Inform Decis Mak. 2024 Jun 21;24(1):177. doi: 10.1186/s12911-024-02579-z. BMC Med Inform Decis Mak. 2024. PMID: 38907265 Free PMC article.
-
Association of Brain Metastases With Survival in Patients With Limited or Stable Extracranial Disease: A Systematic Review and Meta-analysis.JAMA Netw Open. 2023 Feb 1;6(2):e230475. doi: 10.1001/jamanetworkopen.2023.0475. JAMA Netw Open. 2023. PMID: 36821113 Free PMC article.
-
Stereotactic radiosurgery for brain metastases from human epidermal receptor 2 positive breast Cancer: an international, multi-center study.J Neurooncol. 2024 Oct;170(1):199-208. doi: 10.1007/s11060-024-04775-3. Epub 2024 Aug 27. J Neurooncol. 2024. PMID: 39192068 Free PMC article.
References
-
- Johnson JD, Young B. Demographics of brain metastasis. Neurosurg Clin N Am. (1996) 7:337–44. - PubMed
-
- Mehta MP, Tsao MN, Whelan TJ, Morris DE, Hayman JA, Flickinger JC, et al. . The American Society for Therapeutic Radiology and Oncology (ASTRO) evidence-based review of the role of radiosurgery for brain metastases. Int J Radiat Oncol Biol Phys. (2005) 63:37–46. 10.1016/j.ijrobp.2005.05.023 - DOI - PubMed
-
- Borgelt B, Gelber R, Kramer S, Brady LW, Chang CH, Davis LW, et al. . The palliation of brain metastases: final results of the first two studies by the radiation therapy oncology group. Int J Radiat Oncol Biol Phys. (1980) 6:1–9. - PubMed
-
- Leksell L. The stereotaxic method and radiosurgery of the brain. Acta Chir Scand. (1951) 102:316–9. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous