

Autologous Chondrocyte Implantation "Segmental-Sandwich" Technique for Deep Osteochondral Defects in the Knee: Clinical Outcomes and Correlation With Magnetic Resonance Imaging Findings
- PMID: 31192269
- PMCID: PMC6540512
- DOI: 10.1177/2325967119847173
Autologous Chondrocyte Implantation "Segmental-Sandwich" Technique for Deep Osteochondral Defects in the Knee: Clinical Outcomes and Correlation With Magnetic Resonance Imaging Findings
Abstract
Background: Symptomatic osteochondral defects are difficult to manage, especially in patients with deep (>8-10 mm) empty defects. The restoration of articular congruence is crucial to avoid the progression to osteoarthritis (OA).
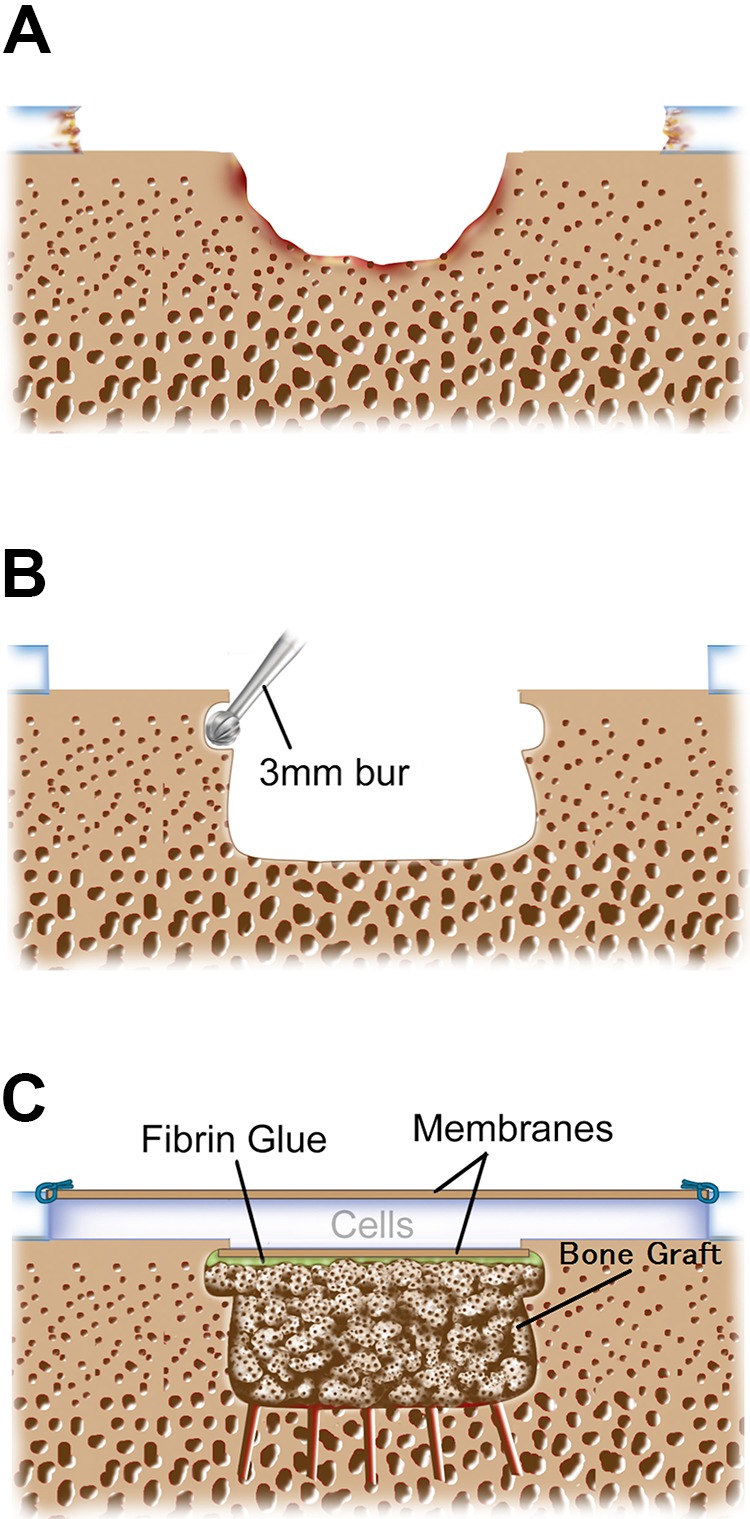
Purpose: To describe the autologous chondrocyte implantation (ACI) "segmental-sandwich" technique for restoration of the osteochondral unit and to evaluate midterm outcomes in patients treated with this procedure. Correlations between magnetic resonance imaging (MRI) and radiographic findings with outcomes were assessed.
Study design: Case series; Level of evidence, 4.
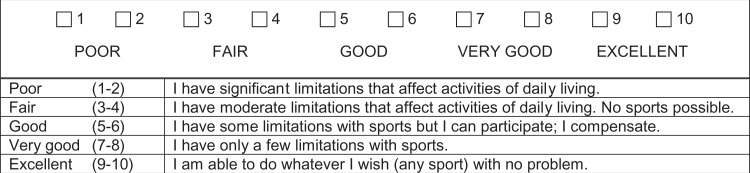
Methods: Outcomes were evaluated for a consecutive cohort of 15 patients with symptomatic deep (>8 mm) osteochondral lesions who underwent autologous bone grafting plus the ACI segmental-sandwich technique performed by a single surgeon between 2003 and 2011. Patients with a minimum 2-year follow-up were included. All patients completed validated clinical outcome scales and a patient satisfaction survey. The Kellgren-Lawrence (K-L) grade was assessed for the progression to OA. The repair site was evaluated with the MOCART (magnetic resonance observation of cartilage repair tissue) score. Filling and tissue characteristics of the bone defect were analyzed with MRI.
Results: All patients (mean age at surgery, 31.0 ± 9.1 years) were available for follow-up (mean follow-up, 7.8 ± 3.0 years; range, 2-15 years). The mean chondral lesion size was 6.0 ± 3.5 cm2 (range, 1.5-13.5 cm2), with a mean bone defect area of 1.7 cm2 (27%-40% of overall surface area treated by ACI) and depth of 1.0 cm. All patients had successful clinical outcomes, and all functional scores improved significantly (P < .05). Patients reported a very high satisfaction rate (93%). The K-L grade demonstrated no significant progression to OA over a mean follow-up of 4.7 years. For 12 patients with MRI results available, the mean MOCART score at a mean of 3.3 years was 64.2 ± 19.9, with complete or near-complete (≥75% of defect volume) chondral defect filling (83%) and complete integration to adjacent cartilage (83%). Bone defects were completely filled in 83% of patients.
Conclusion: The ACI segmental-sandwich technique provides significant functional improvements at midterm follow-up and excellent survival rates. This unique treatment allows for the resurfacing of cartilage defects and the repair of underlying segmental bone lesions.
Keywords: articular; autologous bone graft; autologous chondrocyte implantation; cartilage; osteochondral lesion; osteochondral unit.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: C.S.W. has received consulting fees and educational support from Aastrom Biosciences (contested) and has stock/stock options in Pfizer. T.M. has received consulting fees from Aastrom Biosciences, Conformis, and Vericel and receives royalties from Conformis. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures

Similar articles
-
Autologous Chondrocyte Implantation "Sandwich" Technique Compared With Autologous Bone Grafting for Deep Osteochondral Lesions in the Knee.Am J Sports Med. 2018 Feb;46(2):322-332. doi: 10.1177/0363546517738000. Epub 2017 Nov 10. Am J Sports Med. 2018. PMID: 29125919
-
Autologous Bone Plug Supplemented With Autologous Chondrocyte Implantation in Osteochondral Defects of the Knee.Am J Sports Med. 2016 May;44(5):1249-59. doi: 10.1177/0363546516631739. Epub 2016 Mar 10. Am J Sports Med. 2016. PMID: 26965681
-
Clinical and Radiological Regeneration of Large and Deep Osteochondral Defects of the Knee by Bone Augmentation Combined With Matrix-Guided Autologous Chondrocyte Transplantation.Am J Sports Med. 2017 Nov;45(13):3069-3080. doi: 10.1177/0363546517717679. Epub 2017 Aug 4. Am J Sports Med. 2017. PMID: 28777662
-
[Autologous chondrocyte transplantation with bone augmentation for the treatment of osteochodral defects of the knee : Treatment of osteochondral defects of the femoral condyles using autologous cancellous bone from the iliac crest combined with matrix-guided autologous chondrocyte transplantation].Oper Orthop Traumatol. 2022 Jun;34(3):239-252. doi: 10.1007/s00064-021-00751-6. Epub 2021 Nov 29. Oper Orthop Traumatol. 2022. PMID: 34842942 Free PMC article. Review. German.
-
Clinical and Radiographic Outcomes After Treatment of Patellar Chondral Defects: A Systematic Review.Sports Health. 2021 Sep-Oct;13(5):490-501. doi: 10.1177/19417381211003515. Epub 2021 Apr 22. Sports Health. 2021. PMID: 33885342 Free PMC article.
Cited by
-
Surgical Management of Focal Chondral Defects of the Talus: A Bayesian Network Meta-analysis.Am J Sports Med. 2022 Aug;50(10):2853-2859. doi: 10.1177/03635465211029642. Epub 2021 Sep 20. Am J Sports Med. 2022. PMID: 34543085 Free PMC article.
-
Cartilage Restoration for Isolated Patellar Chondral Defects: An Updated Systematic Review.Orthop J Sports Med. 2023 May 3;11(5):23259671231153422. doi: 10.1177/23259671231153422. eCollection 2023 May. Orthop J Sports Med. 2023. PMID: 37152547 Free PMC article. Review.
-
Reliability of the MOCART score: a systematic review.J Orthop Traumatol. 2021 Oct 6;22(1):39. doi: 10.1186/s10195-021-00603-w. J Orthop Traumatol. 2021. PMID: 34613499 Free PMC article.
-
Knee osteochondritis dissecans-treatment technical aspects.J Orthop. 2022 Aug 11;34:104-110. doi: 10.1016/j.jor.2022.08.005. eCollection 2022 Nov-Dec. J Orthop. 2022. PMID: 36060730 Free PMC article.
-
The Predictive Value of Early Postoperative MRI-Based Bone Marrow Parameters for Mid-Term Outcome after MACI with Autologous Bone Grafting at the Knee.Cartilage. 2022 Jul-Sep;13(3):19476035221093061. doi: 10.1177/19476035221093061. Cartilage. 2022. PMID: 35993371 Free PMC article.
References
-
- Aglietti P, Ciardullo A, Giron F, Ponteggia F. Results of arthroscopic excision of the fragment in the treatment of osteochondritis dissecans of the knee. Arthroscopy. 2001;17(7):741–746. - PubMed
-
- Anderson AF, Pagnani MJ. Osteochondritis dissecans of the femoral condyles: long-term results of excision of the fragment. Am J Sports Med. 1997;25(6):830–834. - PubMed
-
- Assenmacher AT, Pareek A, Reardon PJ, Macalena JA, Stuart MJ, Krych AJ. Long-term outcomes after osteochondral allograft: a systematic review at long-term follow-up of 12.3 years. Arthroscopy. 2016;32(10):2160–2168. - PubMed
-
- Aurich M, Anders J, Trommer T, Liesaus E, Wagner A, Venbrocks R. Autologous chondrocyte transplantation by the sandwich technique. Unfallchirurg. 2007;110(2):176–179. - PubMed
-
- Bartlett W, Gooding CR, Carrington RW, Skinner JA, Briggs TW, Bentley G. Autologous chondrocyte implantation at the knee using a bilayer collagen membrane with bone graft: a preliminary report. J Bone Joint Surg Br. 2005;87(3):330–332. - PubMed
LinkOut - more resources
Full Text Sources
