

Examining the Impact of the Vaginal Birth After Cesarean Risk Calculator Estimation on Trial of Labor After Cesarean Counseling
- PMID: 31192308
- PMCID: PMC6540508
- DOI: 10.1177/2381468319850830
Examining the Impact of the Vaginal Birth After Cesarean Risk Calculator Estimation on Trial of Labor After Cesarean Counseling
Abstract
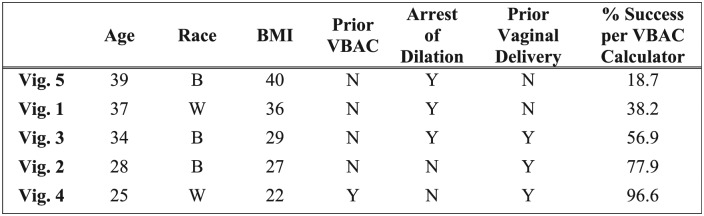
Background. Because failed trial of labor after cesarean (TOLAC) is associated with greater morbidity than planned cesarean, it is important to distinguish women with a high likelihood of successful vaginal birth after cesarean (VBAC) from those likely to fail. The VBAC Calculator may help make this distinction but little is known about how often providers use it; nor whether use improves risk estimation and/or influences TOLAC counseling. Methods. In a cross-sectional survey, a convenience sample of obstetrical providers reported their likelihood (4-point Likert-type scale) to "Recommend,""Offer," or "Agree to" TOLAC for patients presented first through five clinical vignettes; then, in different order, by corresponding VBAC calculator estimates. Results. Of the 85 (of 101, 84% response rate) participants, 88% routinely performed TOLAC, but only 21% used the Calculator. The majority (67.1% to 89.3%) overestimated the likelihood of success for all but one vignette (which had the highest estimate of success). Most providers (42% to 89%) recommended TOLAC for all five vignettes. Given calculated estimates, the majority of providers (67% to 95%) recommended TOLAC for success estimates exceeding 40%. For estimates between 20% and 40%, most providers offered (58%) or agreed (68%) to TOLAC; and even below 20%, over half still agreed to TOLAC. The vignette with the lowest estimate of success (18.7%) had the weakest intraprovider agreement (kappa = 0.116; confidence interval [CI] = 0.045-0.187), whereas the strongest agreement was found in the two vignettes with highest success estimates: 77.9% (kappa = 0.549; CI = 0.382-0.716) and 96.6% (kappa = 0.527; CI = 0.284-0.770). Limitations. Survey responses may not reflect actual practice patterns. Conclusion. Providers are overly optimistic in their clinical estimation of VBAC success. Wider use of decision support could aid in risk stratification and TOLAC counseling to reduce patient morbidity.
Keywords: TOLAC; VBAC; obstetrics; risk estimation.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
Similar articles
-
A Novel and Modern Calculator to Predict Vaginal Birth after Cesarean Delivery.Am J Perinatol. 2025 May 29. doi: 10.1055/a-2605-7786. Online ahead of print. Am J Perinatol. 2025. PMID: 40355120
-
Delivery for women with a previous cesarean: guidelines for clinical practice from the French College of Gynecologists and Obstetricians (CNGOF).Eur J Obstet Gynecol Reprod Biol. 2013 Sep;170(1):25-32. doi: 10.1016/j.ejogrb.2013.05.015. Epub 2013 Jun 28. Eur J Obstet Gynecol Reprod Biol. 2013. PMID: 23810846 Review.
-
Correlates of Trial of Labor and Vaginal Birth After Cesarean in the United States.J Womens Health (Larchmt). 2019 Sep;28(9):1302-1312. doi: 10.1089/jwh.2018.7270. Epub 2019 Mar 13. J Womens Health (Larchmt). 2019. PMID: 30864889
-
[Influencing factors and antenatal assessment of the vaginal birth after cesarean section].Zhonghua Fu Chan Ke Za Zhi. 2019 Jun 25;54(6):369-374. doi: 10.3760/cma.j.issn.0529-567x.2019.06.003. Zhonghua Fu Chan Ke Za Zhi. 2019. PMID: 31262120 Chinese.
-
Trial of labor versus elective repeat cesarean delivery in twin pregnancies after a previous cesarean delivery-A systematic review and meta-analysis.Birth. 2019 Dec;46(4):550-559. doi: 10.1111/birt.12434. Epub 2019 May 23. Birth. 2019. PMID: 31124186
Cited by
-
Effect of a Patient-Centered Decision Support Tool on Rates of Trial of Labor After Previous Cesarean Delivery: The PROCEED Randomized Clinical Trial.JAMA. 2020 Jun 2;323(21):2151-2159. doi: 10.1001/jama.2020.5952. JAMA. 2020. PMID: 32484533 Free PMC article. Clinical Trial.
References
-
- Coleman VH, Erickson K, Schulkin J, Zinberg S, Sachs BP. Vaginal birth after cesarean delivery: practice patterns of obstetrician-gynecologists. J Reprod Med. 2005;50(4):261–6. - PubMed
-
- Armstrong C. ACOG updates recommendations on vaginal birth after previous cesarean delivery. Am Fam Phys. 2011;83(2):215–7.
-
- National Institutes of Health. National Institutes of Health Consensus Development Conference Statement vaginal birth after cesarean: new insights March 8–10, 2010. Semin Perinatol. 2010;34(5):351–65. - PubMed
-
- Grobman WA, Lai Y, Landon MB, et al. National Institute of Child Health and Human Development (NICHD); Maternal-Fetal Medicine Units Network (MFMU). Development of a nomogram for prediction of vaginal birth after cesarean delivery. Obstet Gynecol. 2007;109(4):806–12. - PubMed
LinkOut - more resources
Full Text Sources
