

Using a Health Economic Framework to Prioritize Quality Indicators: An Example With Smoking Cessation in Chronic Obstructive Pulmonary Disease
- PMID: 31192311
- PMCID: PMC6540504
- DOI: 10.1177/2381468319852358
Using a Health Economic Framework to Prioritize Quality Indicators: An Example With Smoking Cessation in Chronic Obstructive Pulmonary Disease
Abstract
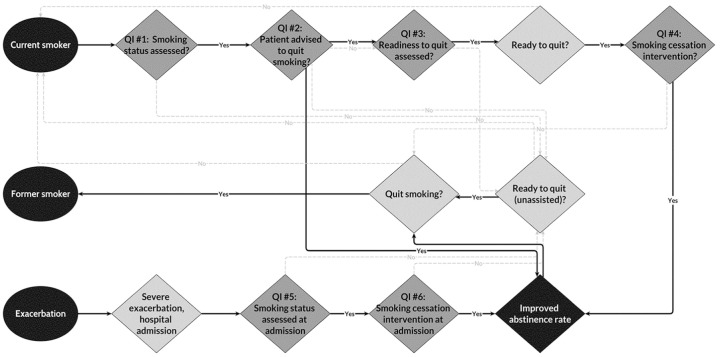
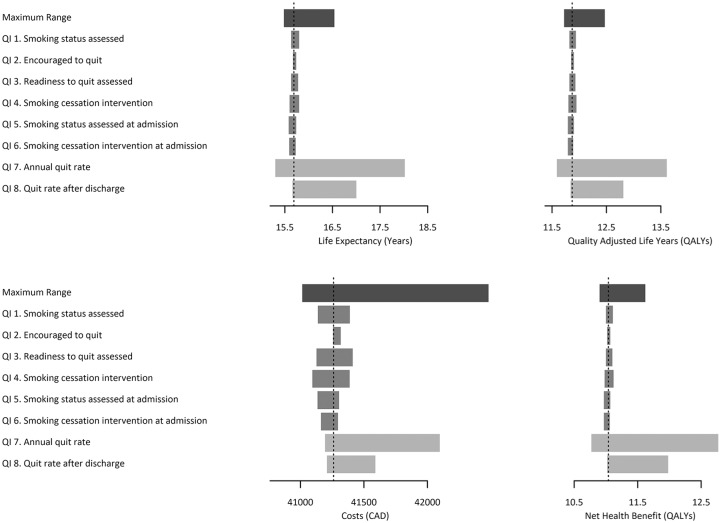
Background. Health care performance monitoring is a major focus of the modern quality movement, resulting in widespread development of quality indicators and making prioritizations an increasing focus. Currently, few prioritization methods of performance measurements give serious consideration to the association of performance with expected health benefits and costs. We demonstrate a proof-of-concept application of using a health economic framework to prioritize quality indicators by expected variations in population health and costs, using smoking cessation in chronic obstructive pulmonary disease (COPD) as an example. Methods. We developed a health state transition, microsimulation model to represent smoking cessation practices for adults with COPD from the health care payer perspective in Ontario, Canada. Variations in life years, quality-adjusted life years (QALYs), and lifetime costs were associated with changes in performance. Incremental net health benefit (INHB) was used to represent the joint variation in mortality, morbidity, and costs associated with the performance of each quality indicator. Results. Using a value threshold of $50,000/QALY, the indicators monitoring assessment of smoking status and smoking cessation interventions were associated with the largest INHBs. Combined performance variations among groups of indicators showed that 81% of the maximum potential INHB could be represented by three out of the six process indicators. Conclusions. A health economic framework can be used to bring dimensions of population health and costs into explicit consideration when prioritizing quality indicators. However, this should not preclude policymakers from considering other dimensions of quality that are not part of this framework.
Keywords: COPD; health economics; quality indicators; smoking cessation.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures

Similar articles
-
Developing and applying a stochastic dynamic population model for chronic obstructive pulmonary disease.Value Health. 2011 Dec;14(8):1039-47. doi: 10.1016/j.jval.2011.06.008. Epub 2011 Sep 22. Value Health. 2011. PMID: 22152172
-
A cost-effectiveness model of smoking cessation based on a randomised controlled trial of varenicline versus placebo in patients with chronic obstructive pulmonary disease.Expert Opin Pharmacother. 2011 Dec;12(17):2613-26. doi: 10.1517/14656566.2011.628935. Epub 2011 Oct 21. Expert Opin Pharmacother. 2011. PMID: 22017336
-
Cost-effectiveness analysis of varenicline versus existing smoking cessation strategies in Central America and the Caribbean using the BENESCO model.Hosp Pract (1995). 2012 Feb;40(1):24-34. doi: 10.3810/hp.2012.02.945. Hosp Pract (1995). 2012. PMID: 22406880
-
The health and economic burden of pertussis in Canada: A microsimulation study.Vaccine. 2019 Nov 20;37(49):7240-7247. doi: 10.1016/j.vaccine.2019.09.070. Epub 2019 Oct 1. Vaccine. 2019. PMID: 31585727
-
Quality-adjusted life-years lack quality in pediatric care: a critical review of published cost-utility studies in child health.Pediatrics. 2005 May;115(5):e600-14. doi: 10.1542/peds.2004-2127. Pediatrics. 2005. PMID: 15867026 Review.
References
-
- Chiu WT, Yang CM, Lin HW, Chu TB. Development and implementation of a nationwide health care quality indicator system in Taiwan. Int J Qual Health Care. 2007;19(1):21–8. - PubMed
-
- Mainz J, Hansen AM, Palshof T, Bartels PD. National quality measurement using clinical indicators: the Danish National Indicator Project. J Surg Oncol. 2009;99(8):500–4. - PubMed
-
- ten Asbroek AHA, Arah OA, Geelhoed J, Custers T, Delnoij DM, Klazinga NS. Developing a national performance indicator framework for the Dutch health system. Int J Qual Health Care. 2004;16(Suppl. 1):i65–i71. - PubMed
-
- Thomson R, Taber S, Lally J, Kazandjian V. UK Quality Indicator Project (UK QIP) and the UK independent health care sector: a new development. Int J Qual Health Care. 2004;16(Suppl. 1):i51–i56. - PubMed
-
- Roland M. Linking physicians’ pay to the quality of care—a major experiment in the United Kingdom. N Engl J Med. 2004;351(14):1448–54. - PubMed
LinkOut - more resources
Full Text Sources
