

Intracochlear Pressure Transients During Cochlear Implant Electrode Insertion: Effect of Micro-mechanical Control on Limiting Pressure Trauma
- PMID: 31192901
- PMCID: PMC6578873
- DOI: 10.1097/MAO.0000000000002164
Intracochlear Pressure Transients During Cochlear Implant Electrode Insertion: Effect of Micro-mechanical Control on Limiting Pressure Trauma
Abstract
Hypothesis: Use of micro-mechanical control during cochlear implant (CI) electrode insertion will result in reduced number and magnitude of pressure transients when compared with standard insertion by hand.
Introduction: With increasing focus on hearing preservation during CI surgery, atraumatic electrode insertion is of the utmost importance. It has been established that large intracochlear pressure spikes can be generated during the insertion of implant electrodes. Here, we examine the effect of using a micro-mechanical insertion control tool on pressure trauma exposures during implantation.
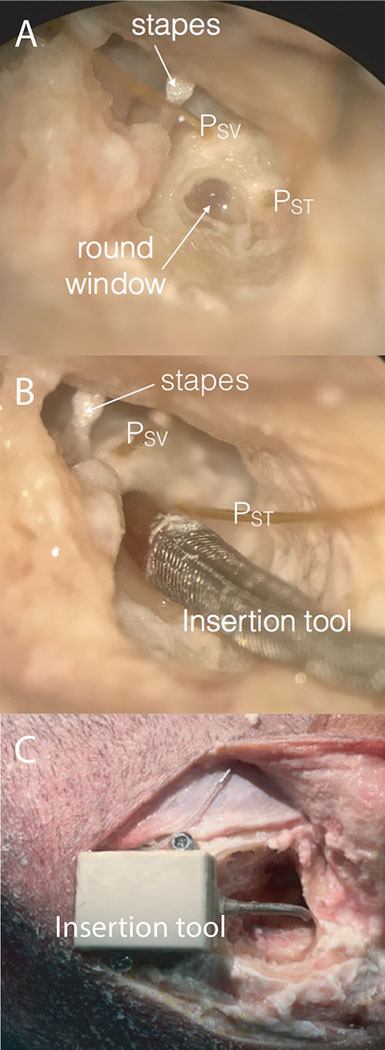
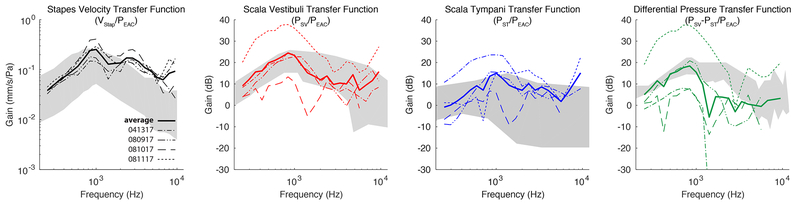
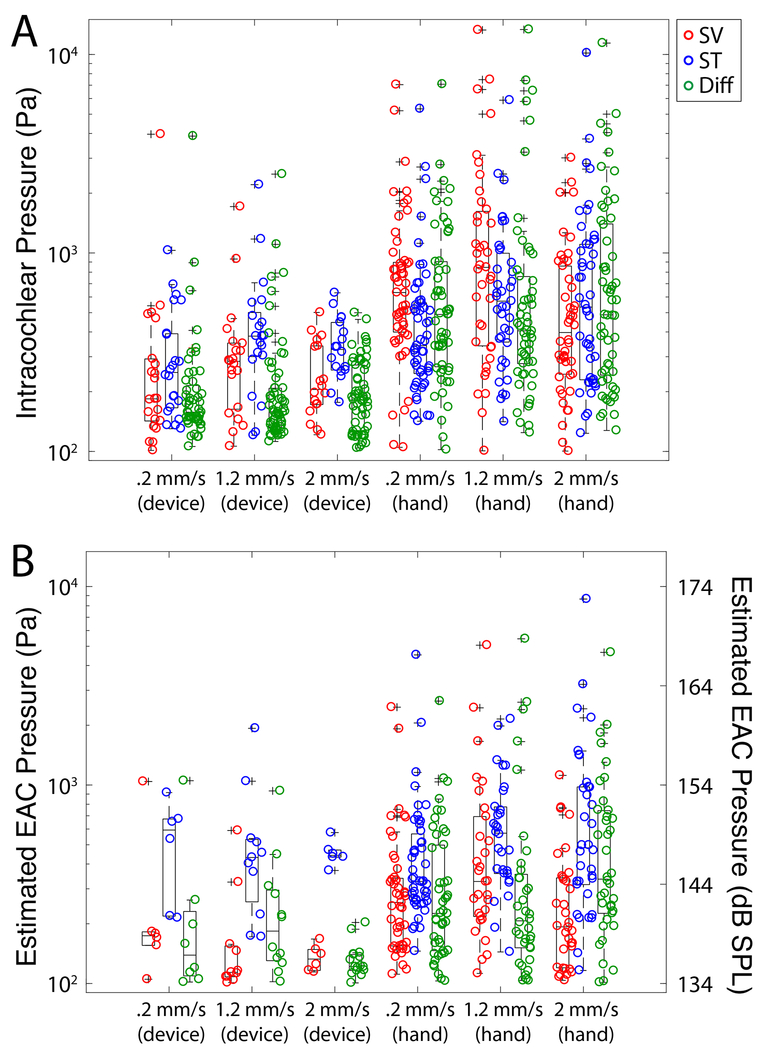
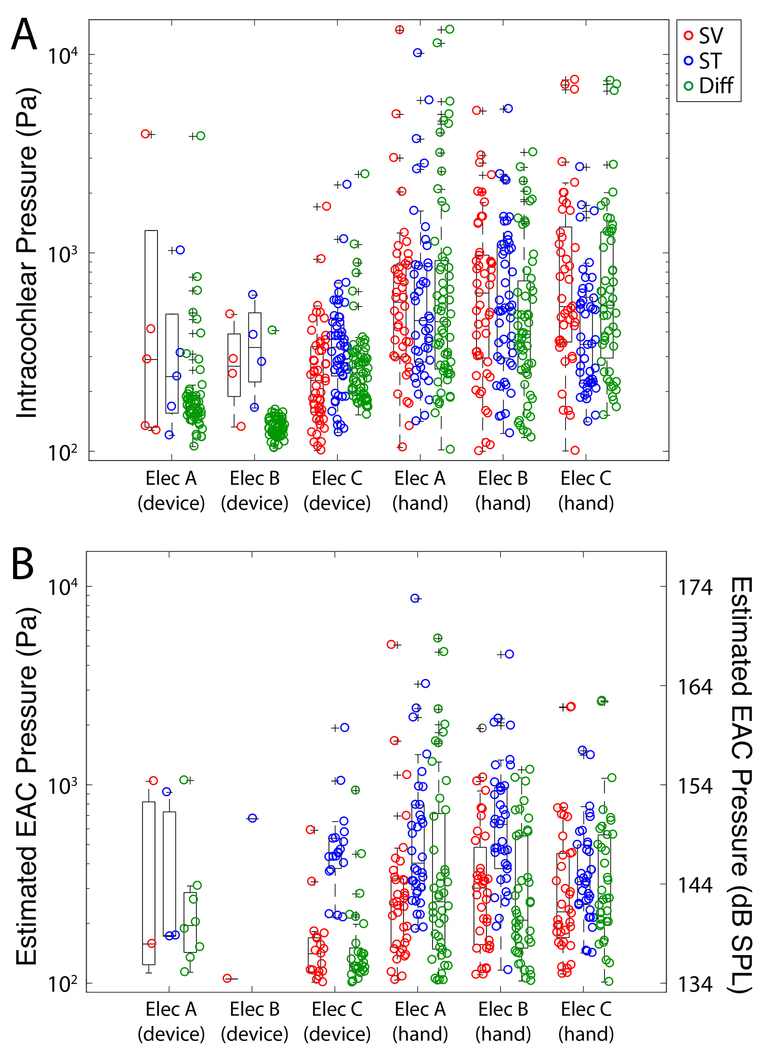
Methods: Human cadaveric heads were surgically prepared with an extended facial recess. Electrodes from three manufacturers were placed both by using a micro-mechanical control tool and by hand. Insertions were performed at three different rates: 0.2 mm/s, 1.2 mm/s, and 2 mm/s (n = 20 each). Fiber-optic sensors measured pressures in scala vestibuli and tympani.
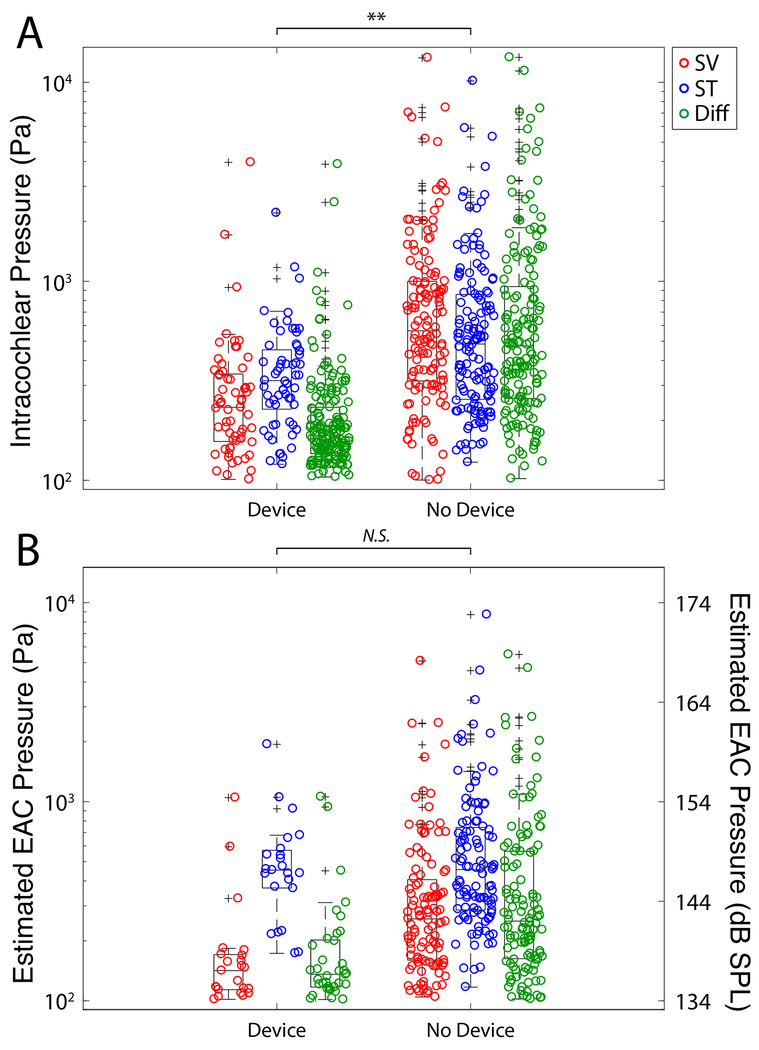
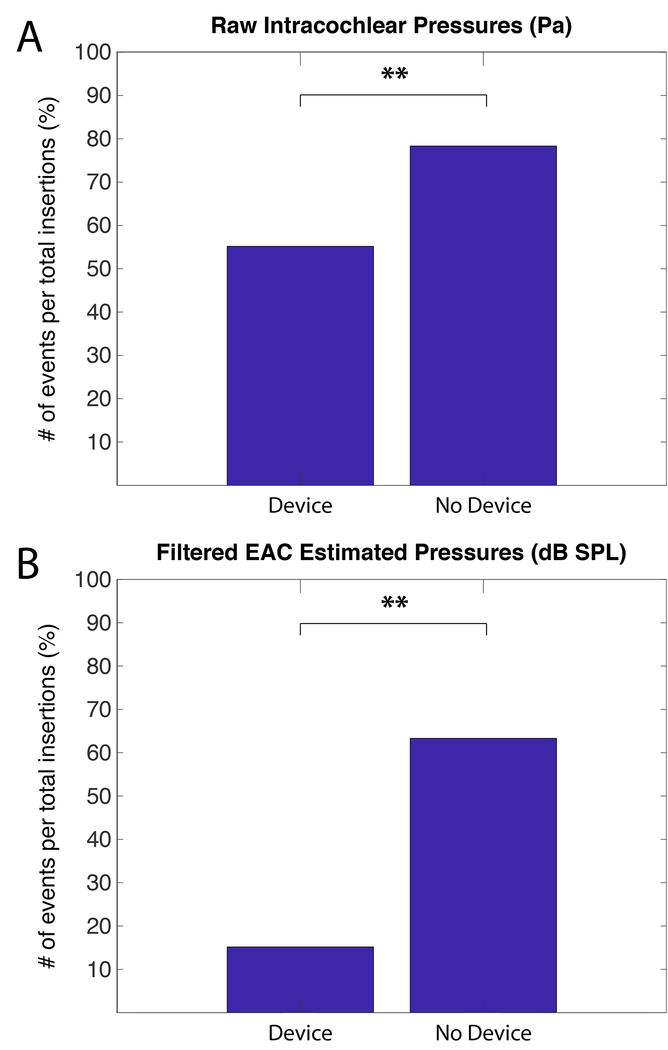
Results: Electrode insertion produced pressure transients up to 174 dB SPL. ANOVA revealed that pressures were significantly lower when using the micro-mechanical control device compared with insertion by hand (p << 0.001). No difference was noted across electrode type or speed. Chi-square analysis showed a significantly lower proportion of insertions contained pressure spikes when the control system was used (p << 0.001).
Conclusion: Results confirm previous data that suggest CI electrode insertion can cause pressure transients with intensities similar to those elicited by high-level sounds. Results suggest that the use of a micro-mechanical insertion control system may mitigate trauma from pressure events, both by reducing the amplitude and the number of pressure spikes resulting from CI electrode insertion.
Conflict of interest statement
Figures
References
-
- Turner CW, Gantz BJ, Vidal C, Behrens A, Henry BA. Speech recognition in noise for cochlear implant listeners: benefits of residual acoustic hearing. J Acoust Soc Am. 2004;115(4):1729–1735. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
