

Incidence of recurrent fungal keratitis after primary keratoplasty and visual outcome and prognosis after intervention for the recurrence
- PMID: 31192926
- PMCID: PMC6587617
- DOI: 10.1097/MD.0000000000015910
Incidence of recurrent fungal keratitis after primary keratoplasty and visual outcome and prognosis after intervention for the recurrence
Abstract
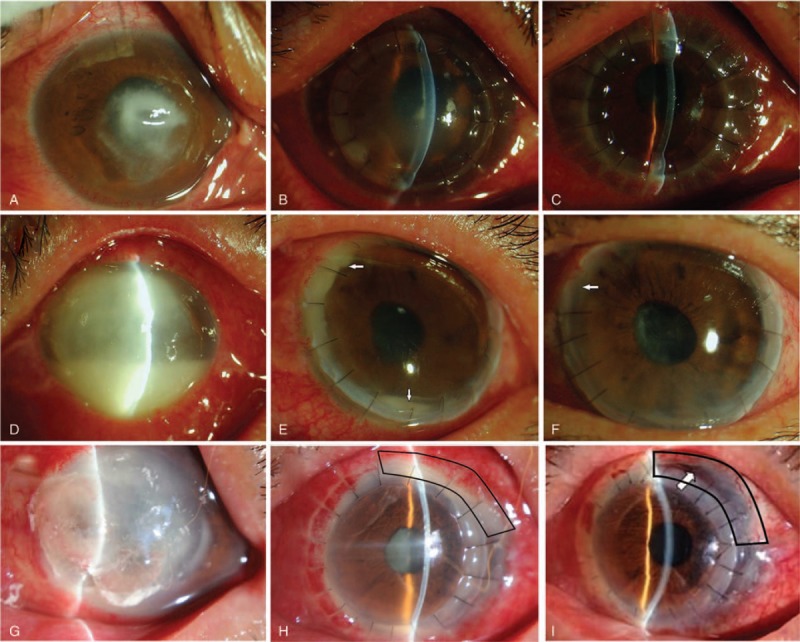
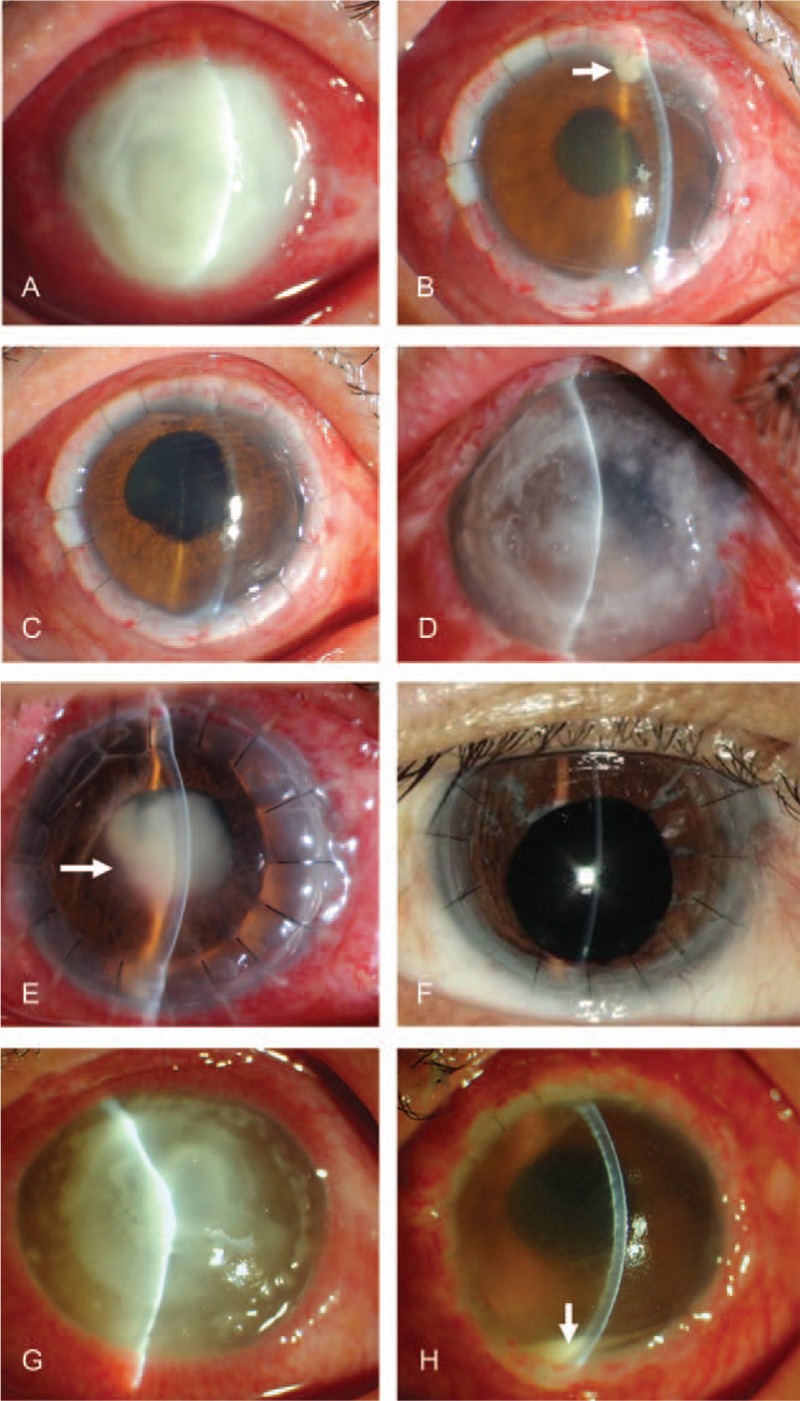
There are no standardized protocols or guidelines for the treatment of recurrent fungal keratitis after therapeutic keratoplasty. This study aimed to investigate the incidence of recurrent fungal keratitis after the primary keratoplasty and the visual outcome and prognosis after intervention for the recurrence.This was a retrospective study. Patients with recurrent fungal keratitis after lamellar keratoplasty (LK) or penetrating keratoplasty (PK) were treated with different antifungal regimens at Shandong Eye Hospital and Qingdao Eye Hospital between Januray 2004 and December 2015. The operative techniques included PK, focal excision, tectonic keratoplasty with a patch graft, lensectomy and vitrectomy, and combined operation. Patients were followed at 1, 2, and 3 months, and then every 6 months after surgery for 2 years. Best corrected visual acuity was assessed and recurrence was recorded. Good prognosis was defined as the presence of visual acuity.Fungal keratitis recurred in 112 of 1448 patients (112/1448, 7.7%) treated initially with PK or LK. The good prognosis rates for different sites of recurrent fungal keratitis were: overall, 93 of 112 (83.0%); recipient bed, 64 of 69 (92.8%); anterior chamber, 14 of 14 (100%); posterior segment, 10 of 16 (62.5%); and atypical, 5 of 13 (38.5%). There was no significant difference in the timing of recurrence between the good and poor prognosis groups (P = .518). Recurrence rates were similar between patients with PK (8.6%) and those with LK (6.0%; P > .05), but the good prognosis rate in patients with post-LK recurrence (96.8%) was higher than that in patients with post-PK recurrence (77.8%, P = .017).Individualized treatment according to recurrent sites of fungal keratitis can achieve a good prognosis in most patients.
Conflict of interest statement
The authors report no conflicts of interest.
Figures
References
-
- Sauer A, Letscher-Bru V, Speeg-Schatz C, et al. In vitro efficacy of antifungal treatment using riboflavin/UV-A (365 nm) combination and amphotericin B. Invest Ophthalmol Vis Sci 2010;51:3950–3. - PubMed
-
- Carrasco MA, Genesoni G. Treatment of severe fungal keratitis with subconjunctival amphotericin B. Cornea 2011;30:608–11. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
