

Minimally invasive triangular osteosynthesis for highly unstable sacral fractures: Technical notes and preliminary clinical outcomes
- PMID: 31192943
- PMCID: PMC6587620
- DOI: 10.1097/MD.0000000000016004
Minimally invasive triangular osteosynthesis for highly unstable sacral fractures: Technical notes and preliminary clinical outcomes
Abstract
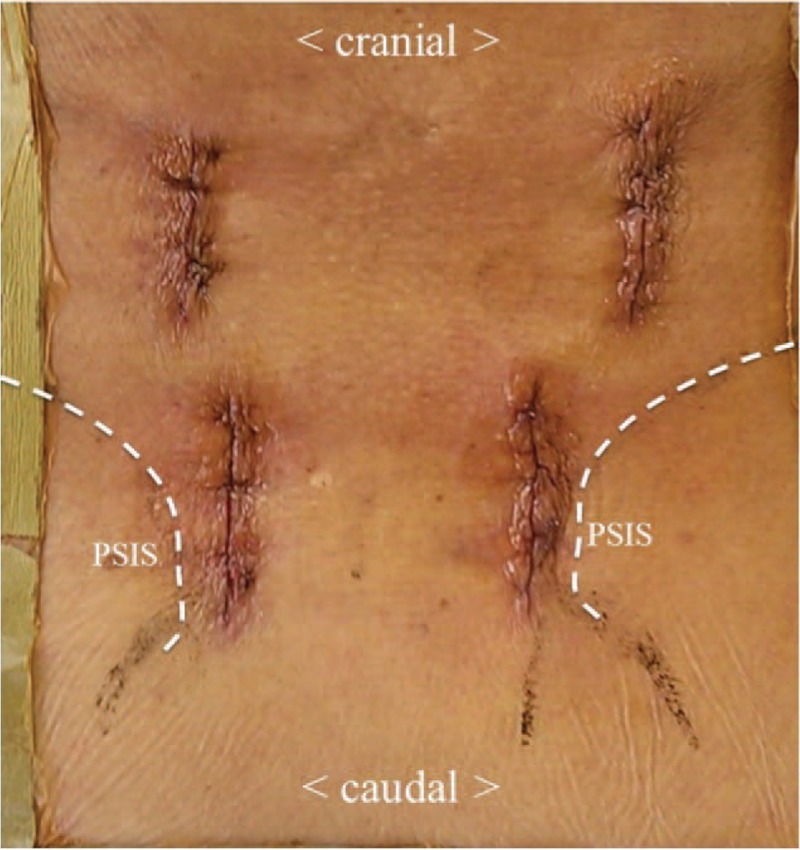
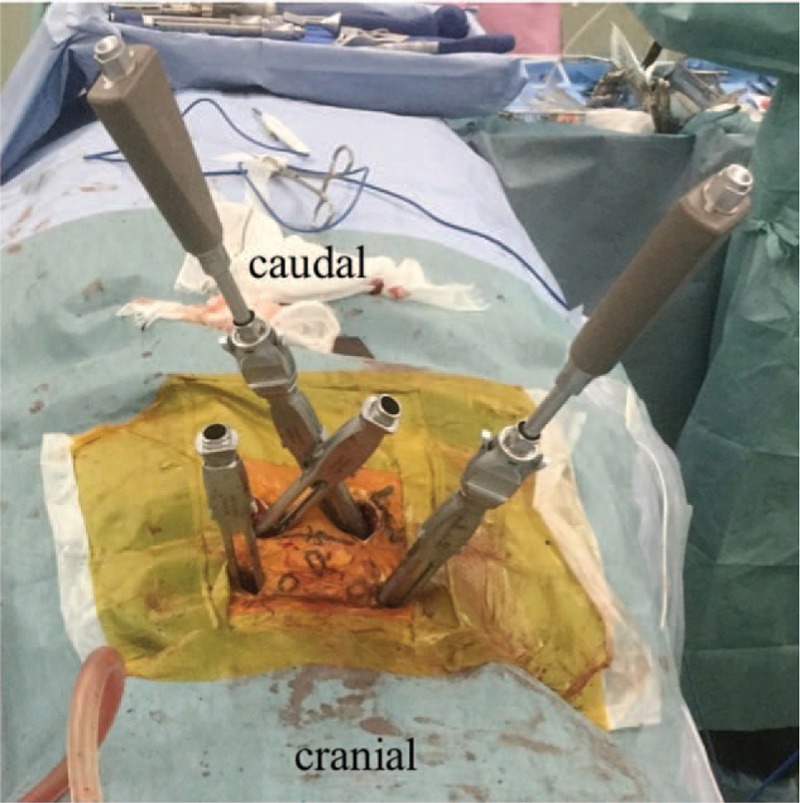
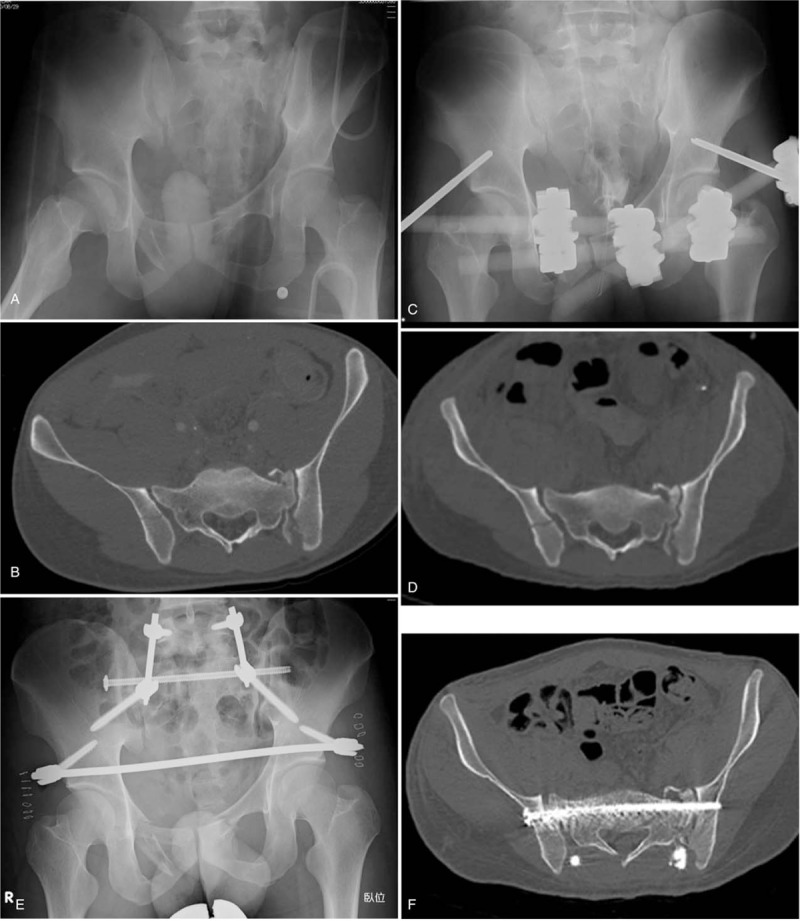
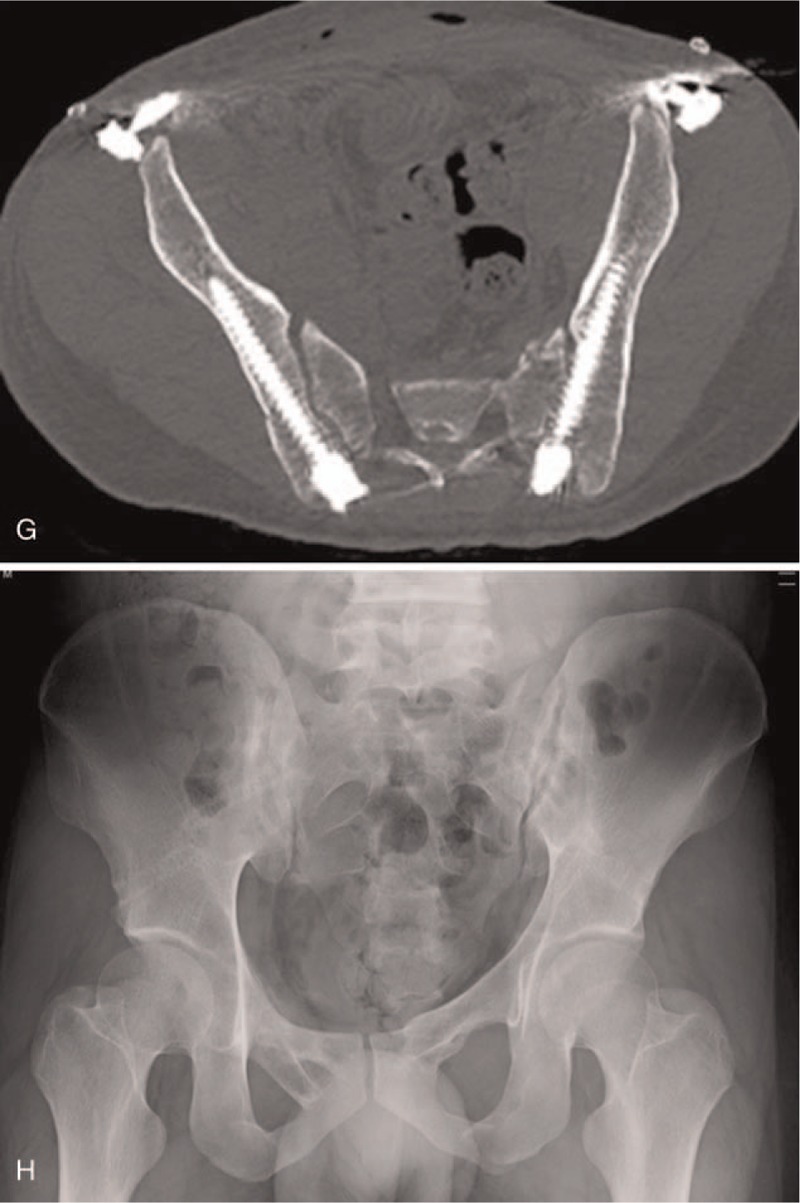
Triangular osteosynthesis involves unilateral L5 iliac posterior instrumentation combined with an iliosacral screw fixation. The aim of this study was to describe this procedure and report the preliminary clinical results in patients with unstable sacral fractures treated with minimally invasive triangular osteosynthesis (MITO). Between 2012 and 2017, 10 patients (6 men and 3 women, mean age, 50 ± 23 years) with sacral fractures were treated with MITO and were followed up for a mean of 15.0 ± 8.5 months in our institution. Classification of sacral fracture, operative time, intraoperative bleeding, timing of full weight bearing, bone union, complications, and clinical outcomes were investigated. Two cases were classified as Denis zone 1, 2 cases as zone 2, and 6 as zone 3. Four patients had Roy-Camille type 1 fracture and 2 patients had type 2. All patients underwent MITO, which involved bilateral lumbopelvic fixation and a uni/bilateral iliosacral screw with stab incisions for percutaneous fixation or central longitudinal incision. The operative time was a mean of 182 ± 64 minutes, and the amount of intraoperative bleeding was a mean of 63 ± 74 g. Full-weight bearing was initiated at a mean of 8.2 ± 2.4 weeks. Eight fractures healed; 1 patient had pulmonary embolism and 1 had implant loosening. Based on Majeed score, 8 patients had "excellent" clinical outcomes, 1 patient had a "good" clinical outcome, and the other had a "fair" clinical outcome. MITO could be less invasive on the soft tissues and be a reliable procedure for bony union. It might provide sufficient stability to accelerate the commencement of post-operative rehabilitation, even in patients with highly unstable sacral fractures.
Conflict of interest statement
Shozo Kanezaki, Masashi Miyazaki, Naoki Notani, Toshinobu Ishihara, Tomonori Sakamoto, Takashi Sone, Masashi Kataoka, and Hiroshi Tsumura declare that they have no conflict of interest.
Figures
Similar articles
-
Robotic guidance for percutaneous placement of triangular osteosynthesis in vertically unstable sacrum fractures: a single-center retrospective study.J Orthop Surg Res. 2023 Jan 4;18(1):8. doi: 10.1186/s13018-022-03489-4. J Orthop Surg Res. 2023. PMID: 36597117 Free PMC article.
-
Comparison of Three-Dimensional Navigation-Guided Percutaneous Iliosacral Screw and Minimally Invasive Percutaneous Plate for the Treatment of Zone II Unstable Sacral Fractures.Orthop Surg. 2023 Feb;15(2):471-479. doi: 10.1111/os.13561. Epub 2022 Dec 2. Orthop Surg. 2023. PMID: 36458444 Free PMC article.
-
A comprehensive analysis with minimum 1-year follow-up of vertically unstable transforaminal sacral fractures treated with triangular osteosynthesis.J Orthop Trauma. 2009 May-Jun;23(5):313-9; discussion 319-21. doi: 10.1097/BOT.0b013e3181a32b91. J Orthop Trauma. 2009. PMID: 19390356 Clinical Trial.
-
[Minimally invasive lumbopelvic stabilization of sacral fracture and sacroiliac injury].Oper Orthop Traumatol. 2021 Dec;33(6):538-545. doi: 10.1007/s00064-021-00730-x. Epub 2021 Sep 1. Oper Orthop Traumatol. 2021. PMID: 34468791 Review. German.
-
Osteosynthesis in sacral fracture and lumbosacral dislocation.Orthop Traumatol Surg Res. 2016 Feb;102(1 Suppl):S45-57. doi: 10.1016/j.otsr.2015.12.002. Epub 2016 Jan 22. Orthop Traumatol Surg Res. 2016. PMID: 26810715 Review.
Cited by
-
A Case Report of a Vertical Zone III Sacral Fracture Due to Acute Lower Extremity Hyperabduction While Windsurfing.Hawaii J Health Soc Welf. 2022 Oct;81(10):267-271. Hawaii J Health Soc Welf. 2022. PMID: 36212222 Free PMC article.
-
Percutaneous posterior transiliac plate versus iliosacral screw fixation for posterior fixation of Tile C-type pelvic fractures: a retrospective comparative study.BMC Musculoskelet Disord. 2022 Jun 16;23(1):581. doi: 10.1186/s12891-022-05536-x. BMC Musculoskelet Disord. 2022. PMID: 35705948 Free PMC article.
-
Robotic guidance for percutaneous placement of triangular osteosynthesis in vertically unstable sacrum fractures: a single-center retrospective study.J Orthop Surg Res. 2023 Jan 4;18(1):8. doi: 10.1186/s13018-022-03489-4. J Orthop Surg Res. 2023. PMID: 36597117 Free PMC article.
-
Biomechanical effects of S1 sacroiliac screws versus S2 sacroiliac screws on sacroiliac screws combined with a lumbar iliac fixation in the treatment of vertical sacral fractures: a biomechanical finite element analysis.BMC Musculoskelet Disord. 2023 Sep 22;24(1):750. doi: 10.1186/s12891-023-06884-y. BMC Musculoskelet Disord. 2023. PMID: 37737168 Free PMC article.
-
Sacral fractures: issues, challenges, solutions.EFORT Open Rev. 2020 May 5;5(5):299-311. doi: 10.1302/2058-5241.5.190064. eCollection 2020 May. EFORT Open Rev. 2020. PMID: 32509335 Free PMC article. Review.
References
-
- Latenser BA, Gentilello LM, Tarver AA, et al. Improved outcome with early fixation of skeletally unstable pelvic fractures. J Trauma 1991;31:28–31. - PubMed
-
- Lykomitros VA, Papavasiliou KA, Alzeer ZM, et al. Management of traumatic sacral fractures: a retrospective case-series study and review of the literature. Injury 2010;41:266–72. - PubMed
-
- Park YS, Baek SW, Kim HS, et al. Management of sacral fractures associated with spinal or pelvic ring injury. J Trauma Acute Care Surg 2012;73:239–42. - PubMed
-
- Nork SE, Jones CB, Harding SP, et al. Percutaneous stabilization of U-shaped sacral fractures using iliosacral screws: technique and early results. J Orthop Trauma 2001;15:238–46. - PubMed
-
- Griffin DR, Starr AJ, Reinert CM, et al. Vertically unstable pelvic fractures fixed with percutaneous iliosacral screws: does posterior injury pattern predict fixation failure? J Orthop Trauma 2003;17:399–405. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
