

Unusual recurrent renal secondary hyperparathyroidism caused by hyperplastic autograft with supernumerary parathyroid adenoma: A case report
- PMID: 31192970
- PMCID: PMC6587644
- DOI: 10.1097/MD.0000000000016077
Unusual recurrent renal secondary hyperparathyroidism caused by hyperplastic autograft with supernumerary parathyroid adenoma: A case report
Abstract
Rationale: Secondary hyperparathyroidism (SHPT) is often complicated with chronic renal failure. Though the total parathyroidectomy (TPTX) with forearm autotransplantation (FAT) has been commonly used to treatment refractory renal SHPT, the recurrence of SHPT is not infrequent, resulting from hyperplastic autograft, remnant parathyroid tissues, and supernumerary parathyroid gland (SPG).
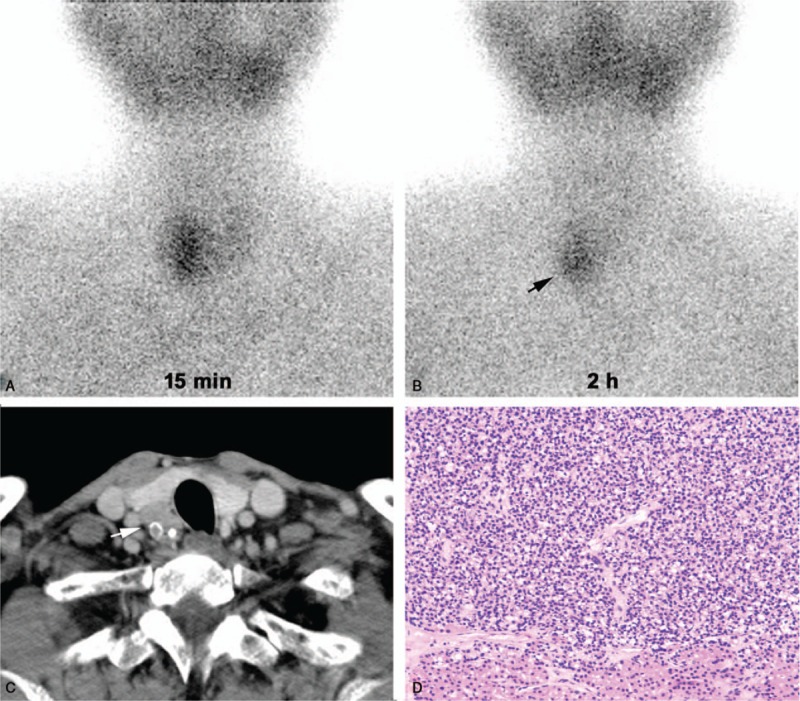
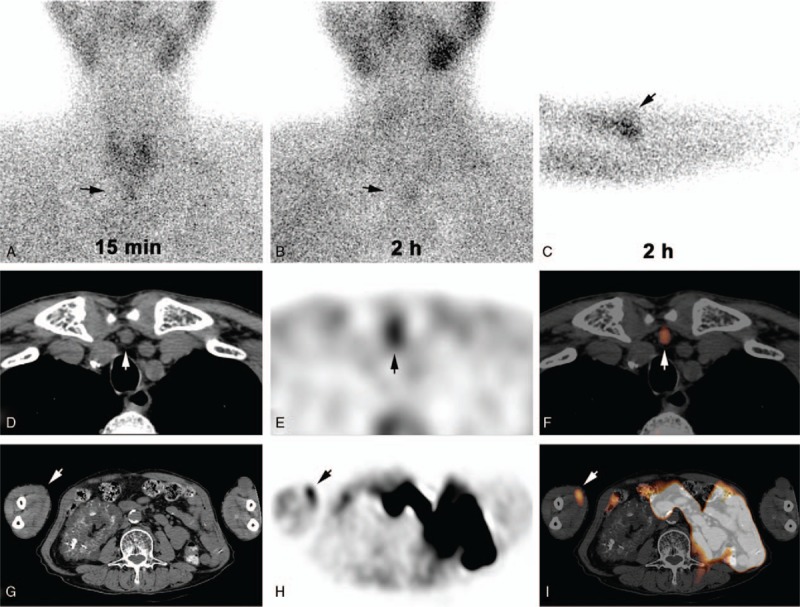
Patient concerns: A 67-year-old man undergoing TPTX+FAT 4 years previously for renal SHPT, who received regular hemodialysis with active vitamin D supplements of Rocaltrol treatment postoperatively, was admitted to our hospital with progressively elevated serum intact parathyroid hormone (iPTH) from 176 to 1266 pg/mL for 8 months and bilateral ankle joints pain for 1 month. Tc-sestamibi dual-phase imaging with single positron emission tomography (SPECT)/computed tomography (CT) revealed a nodule in suprasternal fossa, besides a nodule in autografted site, accompanied with intense radioactivity.
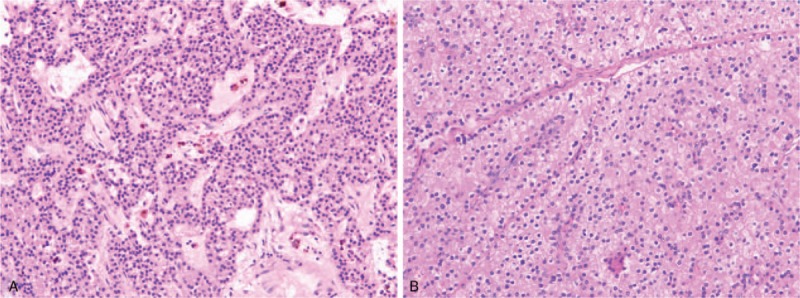
Diagnosis: Recurrent SHPT was easily diagnosed based on previous medical history, painful joints, increased serum iPTH level and positive findings of Tc-sestamibi imaging. Routine postoperative pathology showed that the nodules were consistent with an adenomatoid hyperplasic autograft and a supernumerary parathyroid adenoma in suprasternal fossa, respectively.
Interventions: Reoperation for removing nodules in suprasternal fossa and autografted site was performed 1 month later. Then regular hemodialysis 3 times a week with Rocaltrol was continued.
Outcomes: During 12 months of follow-up, the joints pain improved obviously and the serum iPTH level ranged from 30.1 to 442 pg/mL.
Lessons: Although rare, recurrent renal SHPT may be caused by a coexistence of both hyperfunctional autograft and SPG after TPTX+FAT. The Tc-sestamibi parathyroid imaging with SPECT/CT is helpful to locate the culprits of recurrent renal SHPT before reoperation. To prevent recurrence of renal SHPT, the present initial surgical procedures should be further optimized in patient on permanent hemodialysis.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Recurrent secondary hyperparathyroidism due to a gradually increasing intrathyroidal parathyroid adenoma in a fifth parathyroid gland of a patient undergoing long-term haemodialysis: Road to evil.BMC Nephrol. 2025 Feb 3;26(1):53. doi: 10.1186/s12882-024-03878-3. BMC Nephrol. 2025. PMID: 39901080 Free PMC article.
-
Recurrent renal secondary hyperparathyroidism caused by supernumerary mediastinal parathyroid gland and parathyromatosis: A case report.Front Surg. 2023 Mar 20;10:1135596. doi: 10.3389/fsurg.2023.1135596. eCollection 2023. Front Surg. 2023. PMID: 37021088 Free PMC article.
-
The usefulness of neck pinhole SPECT as a complementary tool to planar scintigraphy in primary and secondary hyperparathyroidism.J Nucl Med. 2004 Jan;45(1):40-8. J Nucl Med. 2004. PMID: 14734671 Clinical Trial.
-
Recurrent or persistent hyperparathyroidism.J Bone Miner Res. 2002 Nov;17 Suppl 2:N158-62. J Bone Miner Res. 2002. PMID: 12412795 Review.
-
Unusual cases of hyperparathyroidism.P R Health Sci J. 1995 Sep;14(3):227-32. P R Health Sci J. 1995. PMID: 8588025 Review.
Cited by
-
A preoperative parathyroid scan is important for the total removal of the transplanted parathyroid tissue in recurrent secondary hyperthyroidism: A case report and literature review.Medicine (Baltimore). 2022 Dec 23;101(51):e32453. doi: 10.1097/MD.0000000000032453. Medicine (Baltimore). 2022. PMID: 36595874 Free PMC article. Review.
References
-
- Fraser WD. Hyperparathyroidism. Lancet 2009;374:145–58. - PubMed
-
- Guideline Working Group JSFD. Clinical practice guideline for the management of secondary hyperparathyroidism in chronic dialysis patients. Ther Apher Dial 2008;12:514–25. - PubMed
-
- Liu ME, Qiu NC, Zha SL, et al. To assess the effects of parathyroidectomy (TPTX versus TPTX+AT) for secondary hyperparathyroidism in chronic renal failure: a systematic review and meta-analysis. Int J Surg 2017;44:353–62. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
