

Use of fenestrated-branched endovascular aneurysm repair to treat Carrel patch aneurysmal degeneration after open thoracoabdominal aortic aneurysm repair
- PMID: 31193425
- PMCID: PMC6529688
- DOI: 10.1016/j.jvscit.2018.12.006
Use of fenestrated-branched endovascular aneurysm repair to treat Carrel patch aneurysmal degeneration after open thoracoabdominal aortic aneurysm repair
Abstract
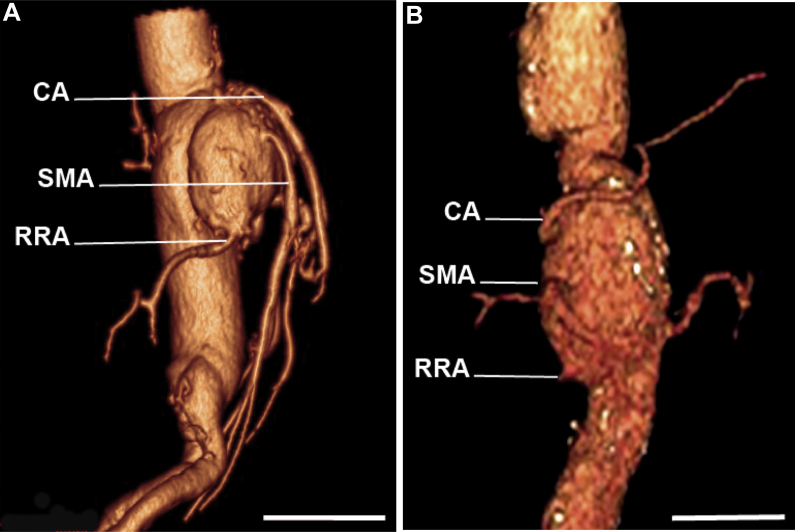
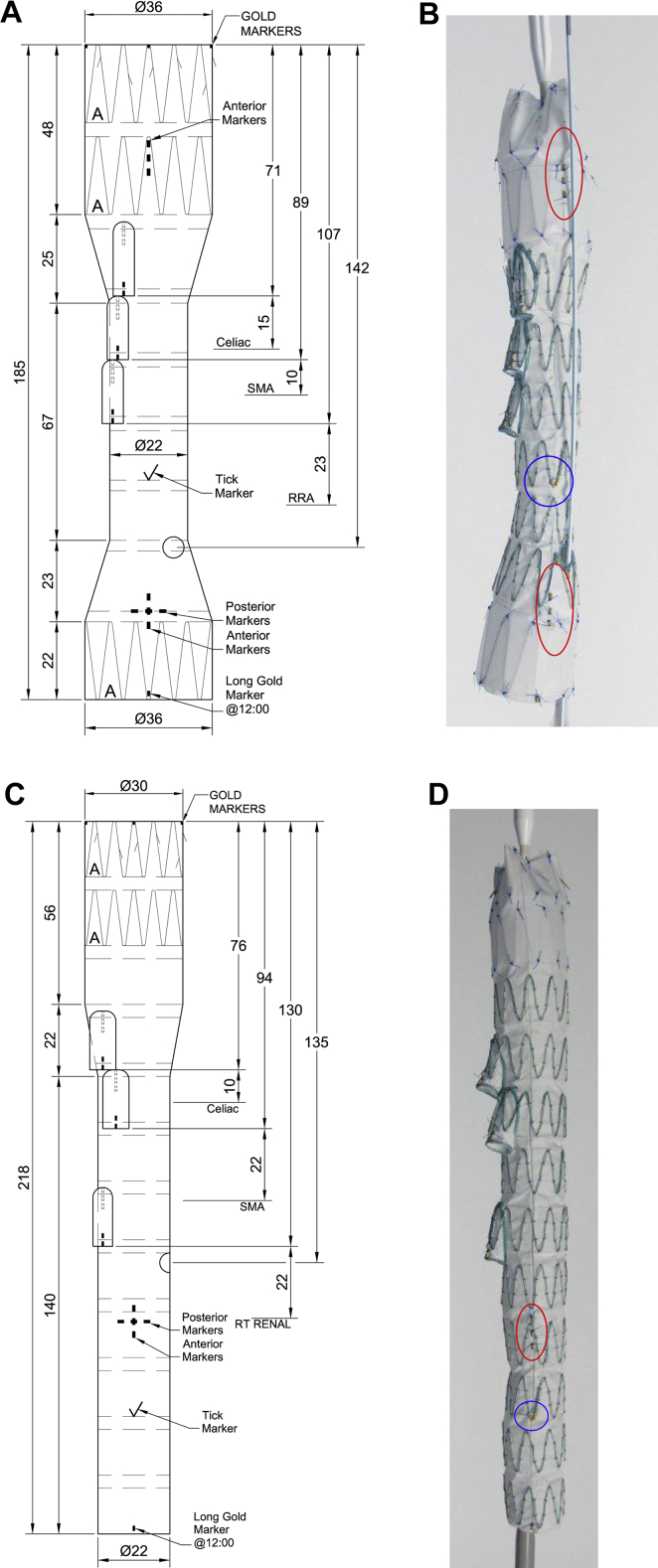
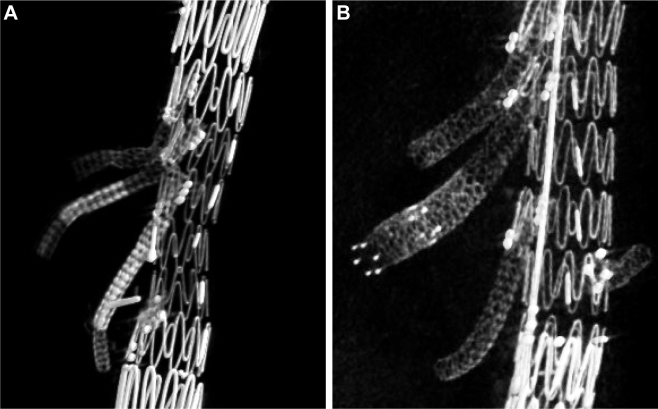
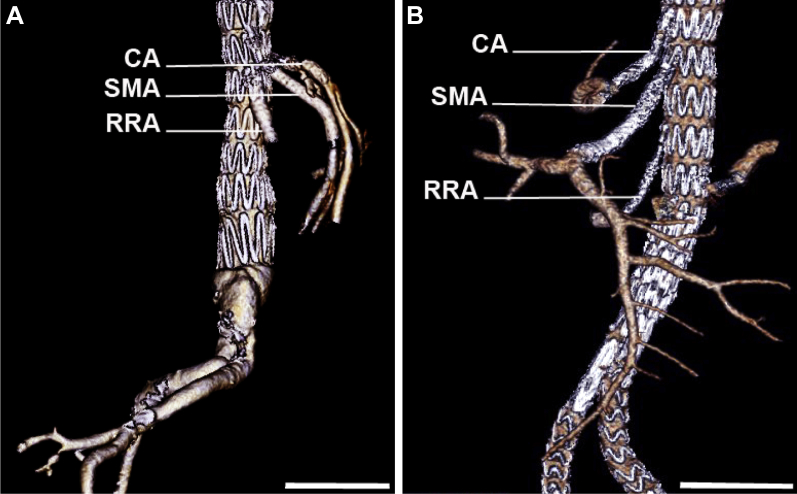
Two patients with a history of open type II thoracoabdominal aortic aneurysm repair presented with saccular aneurysmal degeneration of the Carrel patch. The degenerated segments measured 6.2 cm and 7.4 cm, respectively, and involved the celiac artery, superior mesenteric artery, and right renal artery. Both patients successfully underwent a custom fenestrated-branched endovascular aneurysm repair with downgoing branches to the celiac artery, superior mesenteric artery, and right renal artery and a stented fenestration to the left renal artery. Completion angiography demonstrated no endoleak and patent visceral-renal segments. Both patients were discharged home on postoperative day 2.
Keywords: Aneurysm; Carrel patch; Fenestrated.
Figures
Similar articles
-
Outcomes and complications after fenestrated-branched endovascular aortic repair.J Vasc Surg. 2019 Jul;70(1):15-22. doi: 10.1016/j.jvs.2018.10.052. Epub 2018 Dec 24. J Vasc Surg. 2019. PMID: 30591293
-
Endovascular rescue of a thoracoabdominal fenestrated endograft presenting with combined type 1 and type 3 endoleaks from aortic graft migration and visceral stent separation.Ann Vasc Surg. 2013 Jan;27(1):110.e1-4. doi: 10.1016/j.avsg.2012.05.007. Epub 2012 Oct 23. Ann Vasc Surg. 2013. PMID: 23088803
-
First/Preliminary Experience of Gore Viabahn Balloon-Expandable Endoprosthesis as Bridging Stent in Fenestrated and Branched Endovascular Aortic Repair.Ann Vasc Surg. 2019 Nov;61:299-309. doi: 10.1016/j.avsg.2019.04.049. Epub 2019 Jul 31. Ann Vasc Surg. 2019. PMID: 31376538
-
[Results of endovascular repair of TAAA in the first 50 patients].Zentralbl Chir. 2011 Oct;136(5):451-7. doi: 10.1055/s-0031-1271550. Epub 2011 Jul 15. Zentralbl Chir. 2011. PMID: 21766273 Review. German.
-
A modified technique of intercostal artery implantation for thoracoabdominal aortic aneurysm using the tube of the aortic wall.Ann Vasc Dis. 2013;6(3):662-5. doi: 10.3400/avd.cr.13-00049. Epub 2013 Aug 12. Ann Vasc Dis. 2013. PMID: 24130626 Free PMC article. Review.
Cited by
-
Parallel intercostal artery stenting and exclusion of symptomatic bucket-handle intercostal patch aneurysm.J Vasc Surg Cases Innov Tech. 2024 Mar 18;10(3):101486. doi: 10.1016/j.jvscit.2024.101486. eCollection 2024 Jun. J Vasc Surg Cases Innov Tech. 2024. PMID: 38650759 Free PMC article.
References
-
- Carrel T.P., Signer C. Separate revascularization of the visceral arteries in thoracoabdominal aneurysm repair. Ann Thorac Surg. 1999;68:573–575. - PubMed
-
- Crawford E.S., Schuessler J.S. Thoracoabdominal and abdominal aortic aneurysms involving celiac, superior mesenteric, and renal arteries. World J Surg. 1980;4:643–651. - PubMed
-
- Elefteriades J.A. Natural history of thoracic aortic aneurysms: indications for surgery, and surgical versus nonsurgical risks. Ann Thorac Surg. 2002;74:S1877–S1880. discussion: S1892-8. - PubMed
-
- Griepp R.B., Ergin M.A., Galla J.D., Lansman S.L., McCollough J.N., Nguyen K.H. Natural history of descending thoracic and thoracoabdominal aneurysms. Ann Thorac Surg. 1999;67:1927–1930. discussion: 1953-8. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
