

Meta-analytic Evidence for the Plurality of Mechanisms in Transdiagnostic Structural MRI Studies of Hallucination Status
- PMID: 31193632
- PMCID: PMC6537703
- DOI: 10.1016/j.eclinm.2019.01.012
Meta-analytic Evidence for the Plurality of Mechanisms in Transdiagnostic Structural MRI Studies of Hallucination Status
Abstract
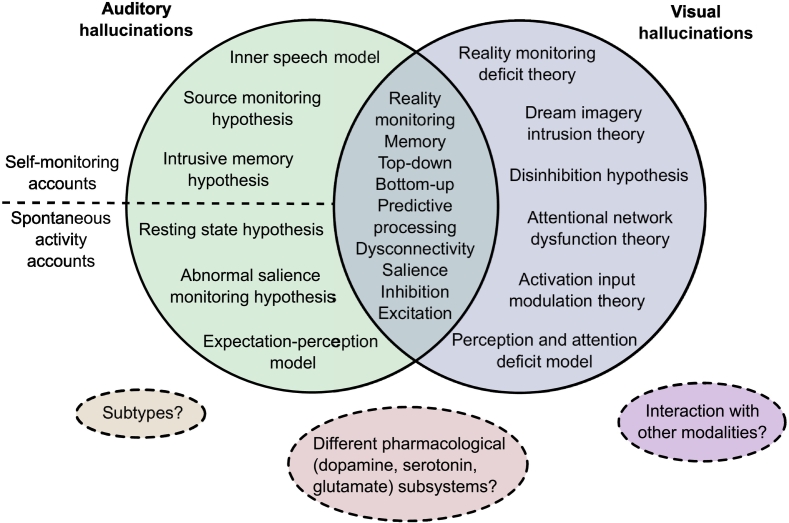
Background: Hallucinations are transmodal and transdiagnostic phenomena, occurring across sensory modalities and presenting in psychiatric, neurodegenerative, neurological, and non-clinical populations. Despite their cross-category occurrence, little empirical work has directly compared between-group neural correlates of hallucinations.
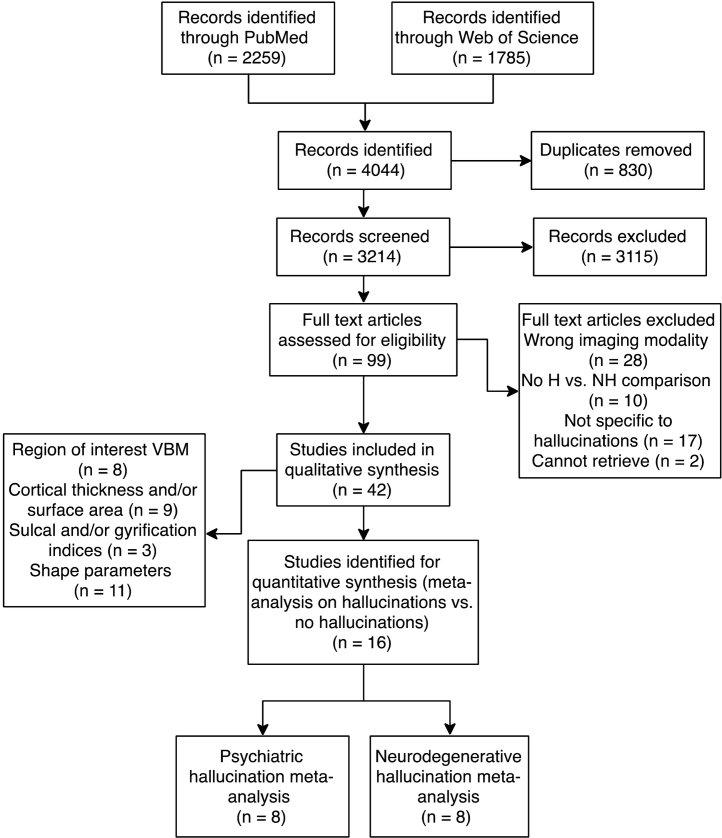
Methods: We performed whole-brain voxelwise meta-analyses of hallucination status across diagnoses using anisotropic effect-size seed-based d mapping (AES-SDM), and conducted a comprehensive systematic review in PubMed and Web of Science until May 2018 on other structural correlates of hallucinations, including cortical thickness and gyrification.
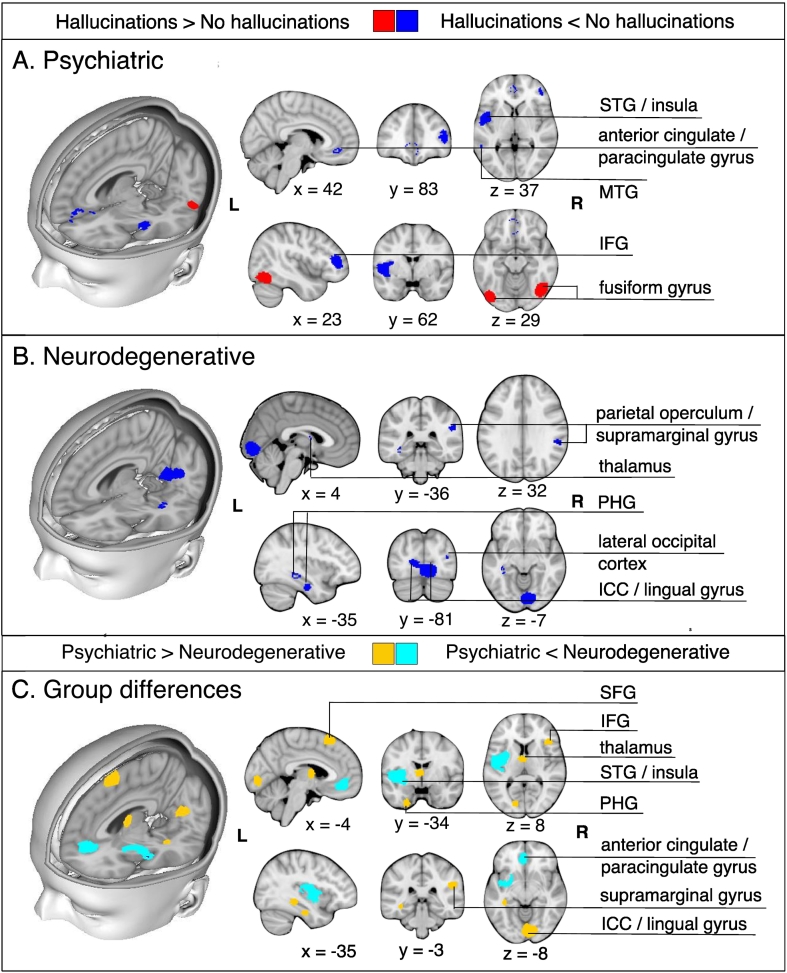
Findings: 3214 abstracts were identified. Patients with psychiatric disorders and hallucinations (eight studies) exhibited reduced gray matter (GM) in the left insula, right inferior frontal gyrus, left anterior cingulate/paracingulate gyrus, left middle temporal gyrus, and increased in the bilateral fusiform gyrus, while patients with neurodegenerative disorders with hallucinations (eight studies) showed GM decreases in the left lingual gyrus, right supramarginal gyrus/parietal operculum, left parahippocampal gyrus, left fusiform gyrus, right thalamus, and right lateral occipital gyrus. Group differences between psychiatric and neurodegenerative hallucination meta-analyses were formally confirmed using Monte Carlo randomizations to determine statistical significance, and a jackknife sensitivity analysis established the reproducibility of results across nearly all study combinations. For other structural measures (28 studies), the most consistent findings associated with hallucination status were reduced cortical thickness in temporal gyri in schizophrenia and altered hippocampal volume in Parkinson's disease and dementia. Additionally, increased severity of hallucinations in schizophrenia correlated with GM reductions within the left superior temporal gyrus, right middle temporal gyrus, bilateral supramarginal and angular gyri.
Interpretation: Distinct patterns of neuroanatomical alteration characterize hallucination status in patients with psychiatric and neurodegenerative diseases, suggesting a plurality of anatomical signatures. This approach has implications for treatment, theoretical frameworks, and generates refutable predictions for hallucinations in other diseases and their occurrence within the general population.
Funding: None.
Keywords: Hallucination; Meta-analysis; Neurodegenerative; Psychiatric; Structural MRI; Systematic review; Transdiagnostic.
Conflict of interest statement
Ms. Rollins reports a scholarship from Gates Cambridge during the conduct of the study. Professor Rowe reports grants from Wellcome Trust during the conduct of the study, grants from NIHR, McDonnell Foundation, PSP Association, Parkinsons UK, Medical Research Council, Evelyn Trust, and AZ-Medimmune, personal fees from Asceneuron, and other from Guarantors of Brain outside the submitted work. Professor Suckling, Dr. Murray, Dr. Garrison, Dr. Simons, and Dr. O'Callaghan have nothing to disclose.
Figures
References
-
- Lim A., Hoek H.W., Deen M.L., Blom J.D., Investigators G. Prevalence and classification of hallucinations in multiple sensory modalities in schizophrenia spectrum disorders. Schizophr Res. 2016;176(2–3):493–499. - PubMed
-
- Baethge C., Baldessarini R.J., Freudenthal K., Streeruwitz A., Bauer M., Bschor T. Hallucinations in bipolar disorder: characteristics and comparison to unipolar depression and schizophrenia. Bipolar Disord. 2005;7(2):136–145. - PubMed
-
- Diederich N.J., Fenelon G., Stebbins G., Goetz C.G. Hallucinations in Parkinson disease. Nat Rev Neurol. 2009;5(6):331–342. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
