

Proactive Peer (Mother-to-Mother) Breastfeeding Support by Telephone (Ringing up About Breastfeeding Early [RUBY]): A Multicentre, Unblinded, Randomised Controlled Trial
- PMID: 31193656
- PMCID: PMC6537529
- DOI: 10.1016/j.eclinm.2019.02.003
Proactive Peer (Mother-to-Mother) Breastfeeding Support by Telephone (Ringing up About Breastfeeding Early [RUBY]): A Multicentre, Unblinded, Randomised Controlled Trial
Abstract
Background: Breastfeeding rates are suboptimal internationally, and many infants are not receiving any breast milk at all by six months of age. Few interventions increase breastfeeding duration, particularly where there is relatively high initiation. The effect of proactive peer (mother-to-mother) support has been found to increase breastfeeding in some contexts but not others, but if it is shown to be effective would be a potentially sustainable model in many settings. We aimed to determine whether proactive telephone-based peer support during the postnatal period increases the proportion of infants being breastfed at six months of age.
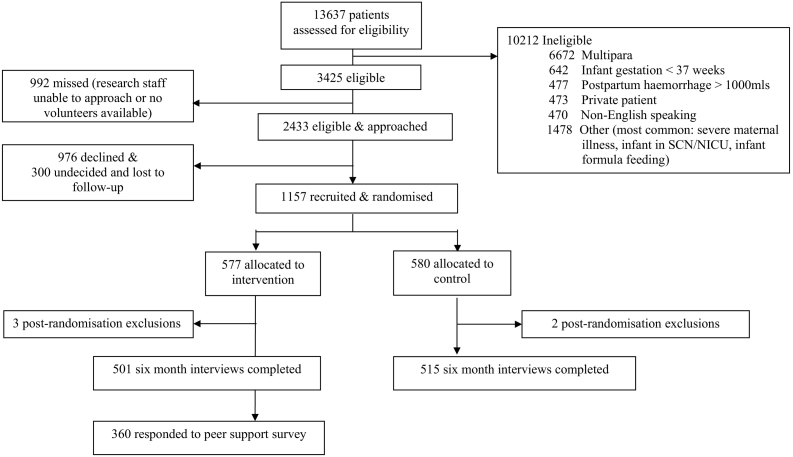
Methods: RUBY (Ringing Up about Breastfeeding earlY) was a multicentre, two-arm un-blinded randomised controlled trial conducted in three hospitals in Victoria, Australia. First-time mothers intending to breastfeed were recruited after birth and prior to hospital discharge, and randomly assigned (1:1) to usual care or usual care plus proactive telephone-based breastfeeding support from a trained peer volunteer for up to six months postpartum. A computerised random number program generated block sizes of four or six distributed randomly, with stratification by site. Research midwives were masked to block size, but masking of allocation was not possible. The primary outcome was the proportion of infants receiving any breast milk at six months of age. Analyses were by intention to treat; data were collected and analysed masked to group. The trial is registered with ACTRN, number 12612001024831.
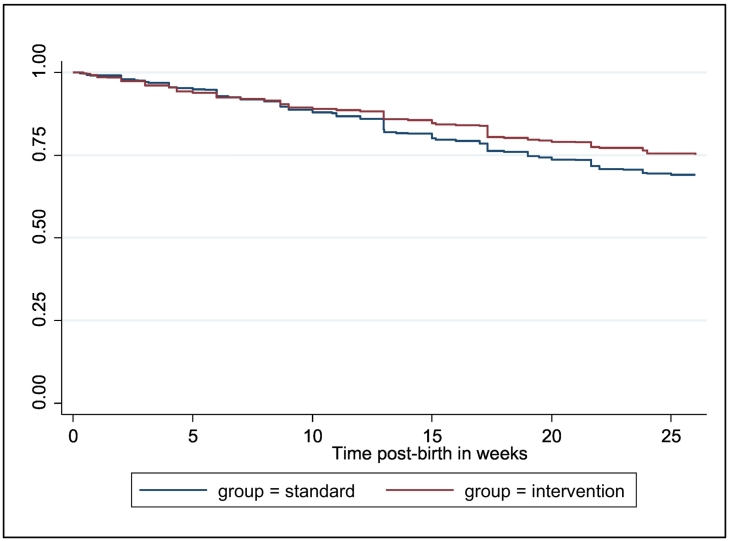
Findings: Women were recruited between Feb 14, 2013 and Dec 15, 2015 and randomly assigned to peer support (n = 574) or usual care (n = 578). Five were not in the primary analysis [5 post-randomisation exclusions]. Infants of women allocated to telephone-based peer support were more likely than those allocated to usual care to be receiving breast milk at six months of age (intervention 75%, usual care 69%; Adj. RR 1·10; 95% CI 1·02, 1·18). There were no adverse events.
Interpretation: Providing first time mothers with telephone-based support from a peer with at least six months personal breastfeeding experience is an effective intervention for increasing breastfeeding maintenance in settings with high breastfeeding initiation.
Funding: The Felton Bequest, Australia, philanthropic donation and La Trobe University grant.
Keywords: ABA, Australian Breastfeeding Association; ACTRN, Australian New Zealand Clinical Trials Registry number; AUD, Australian dollar(s); Adj. RR, Adjusted relative risk; Breastfeeding; CI, Confidence interval; Clinical trial; Community-based; HR, Hazard ratio; Peer support; Peer volunteer; RCT, Randomised controlled trial; RR, Relative risk; RUBY, Ringing Up about Breastfeeding earlY; Telephone intervention; sd, Standard deviation.
Conflict of interest statement
We declare there are no competing interests. Funding was received from the Felton Bequest for the study, and a PhD scholarship was provided by La Trobe University.
Figures
References
-
- Victora C.G., Bahl R., Barros A.J. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet. 2016;387(10017):475–490. - PubMed
-
- Rollins N.C., Bhandari N., Hajeebhoy N. Why invest, and what it will take to improve breastfeeding practices? Lancet. 2016;387(10017):491–504. - PubMed
-
- Sankar M.J., Sinha B., Chowdhury R. Optimal breastfeeding practices and infant and child mortality: a systematic review and meta-analysis. Acta Paediatr Suppl. 2015;104(467):3–13. - PubMed
-
- Australian Institute of Health and Welfare . AIHW; Canberra: 2011. 2010 Australian National Infant Feeding Survey: indicator results.
LinkOut - more resources
Full Text Sources
Research Materials
