

Changing the System - Major Trauma Patients and Their Outcomes in the NHS (England) 2008-17
- PMID: 31193723
- PMCID: PMC6537569
- DOI: 10.1016/j.eclinm.2018.07.001
Changing the System - Major Trauma Patients and Their Outcomes in the NHS (England) 2008-17
Abstract
Background: Trauma care in England was re-organised in 2012 with ambulance bypass of local hospitals to newly designated Major Trauma Centres (MTCs). There is still controversy about the optimal way to organise health series for patients suffering severe injury.
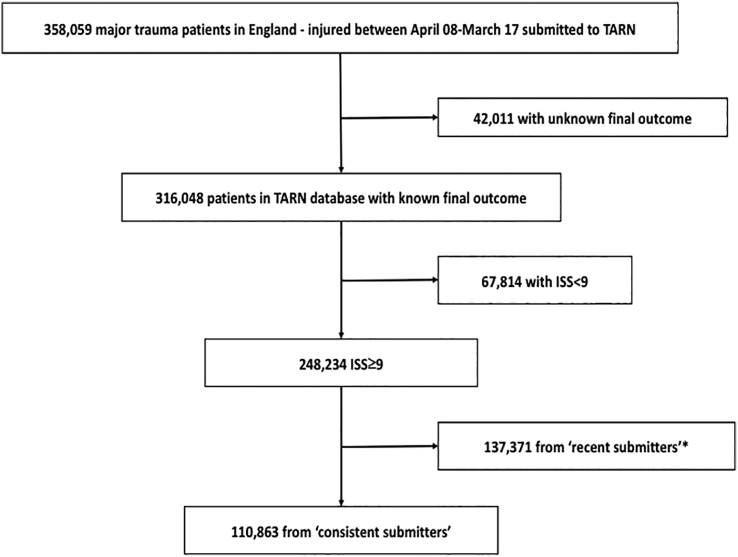
Methods: A longitudinal series of annual cross-sectional studies of care process and outcomes from April 2008 to March 2017. Data was collected through the national clinical audit of major trauma care. The primary analysis was carried out on the 110,863 patients admitted to 35 hospitals that were 'consistent submitters' throughout the study period. The main outcome was longitudinal analysis of risk adjusted survival.
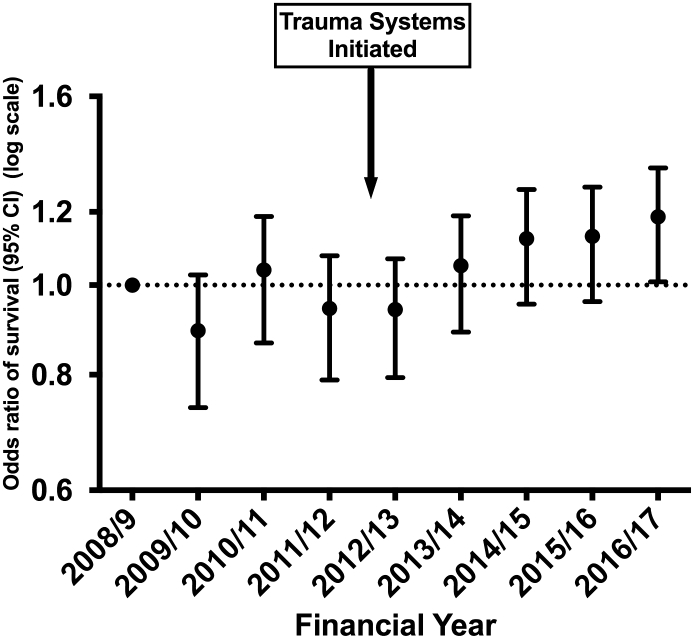
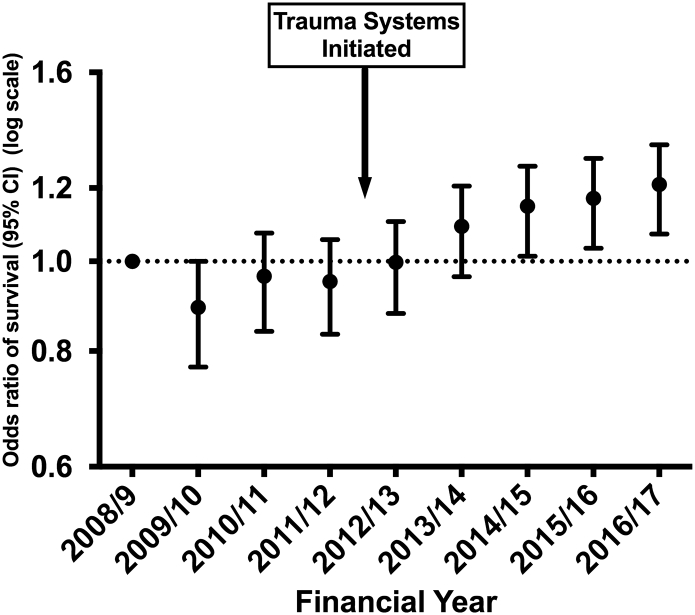
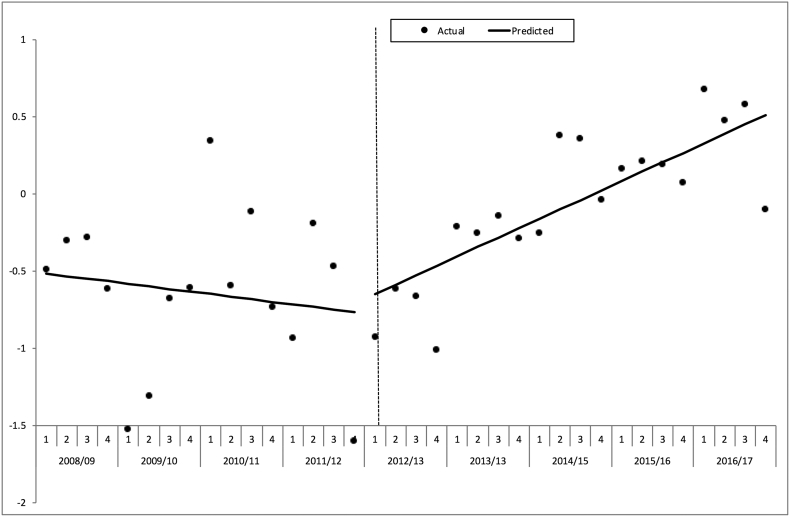
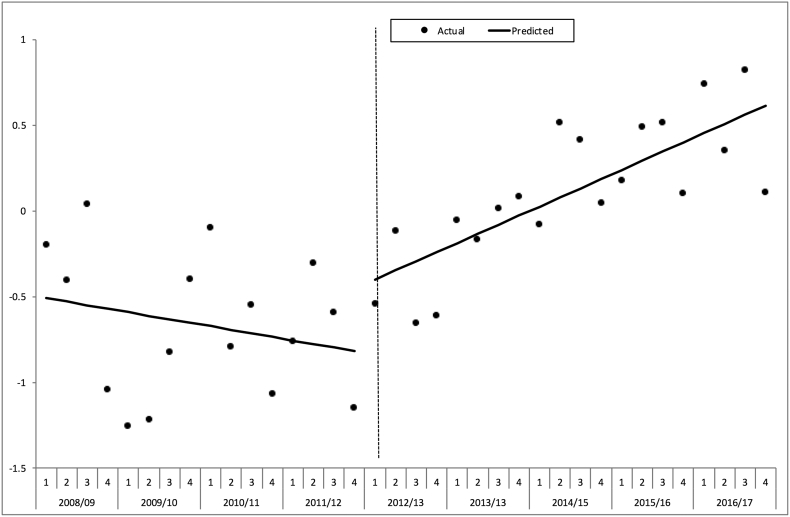
Findings: Major Trauma networks were associated with significant changes in (1) patient flow (with increased numbers treated in Major Trauma Centres), (2) treatment systems (more consultant led care and more rapid imaging), (3) patient factors (an increase in older trauma), and (4) clinical care (new massive transfusion policies and use of tranexamic acid). There were 10,247 (9.2%) deaths in the 110,863 patients with an ISS of 9 or more. There were no changes in unadjusted mortality. The analysis of trends in risk adjusted survival for study hospitals shows a 19% (95% CI 3%-36%) increase in the case mix adjusted odds of survival from severe injury over the 9-year study period. Interrupted time series analysis showed a significant positive change in the slope after the intervention time point of April 2012 (+ 0.08% excess survivors per quarter, p = 0.023), in other words an increase of 0.08 more survivors per 100 patients every quarter.
Interpretation: A whole system national change was associated with significant improvements in both the care process and outcomes of patients after severe injury.
Funding: This analysis was carried out independently and did not receive funding. The data collection for the national clinical audit was funded by subscriptions from participating hospitals.
Keywords: Major trauma; Trauma systems; Wounds and injuries.
Figures
References
-
- CJL Murray, Vos T., Lozano R. Disability-adjusted life years (DALYs) for 291 diseases and injuries in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2197–2223. - PubMed
-
- Ruchholtz S., Mand C., Lewan U. Regionalisation of trauma care in Germany: the “TraumaNetwork DGU(A (R))-project”. Eur J Trauma Emerg Surg. 2012;38(1):11–17. - PubMed
-
- Gabbe B.J., Simpson P.M., Sutherland A.M. Improved functional outcomes for major trauma patients in a regionalized, inclusive trauma system. Ann Surg. 2012;255(6):1009–1015. - PubMed
-
- Gruen R.L., Gabbe B.J., Stelfox H.T. Indicators of the quality of trauma care and the performance of trauma systems. Br J Surg. 2012;99:97–104. - PubMed
-
- Trunkey D.D. Trauma centers and trauma systems. JAMA-J Am Med Assoc. 2003;289(12):1566–1567. - PubMed
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
