

Benign positional vertigo, its diagnosis, treatment and mimics
- PMID: 31193795
- PMCID: PMC6542326
- DOI: 10.1016/j.cnp.2019.03.001
Benign positional vertigo, its diagnosis, treatment and mimics
Abstract
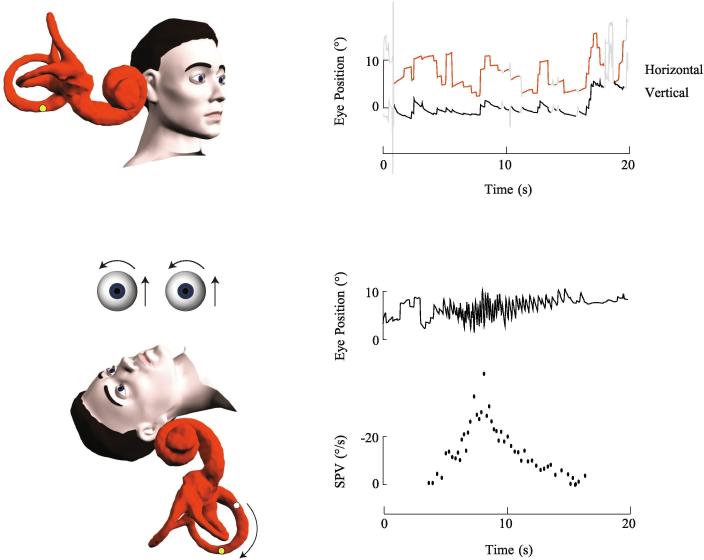
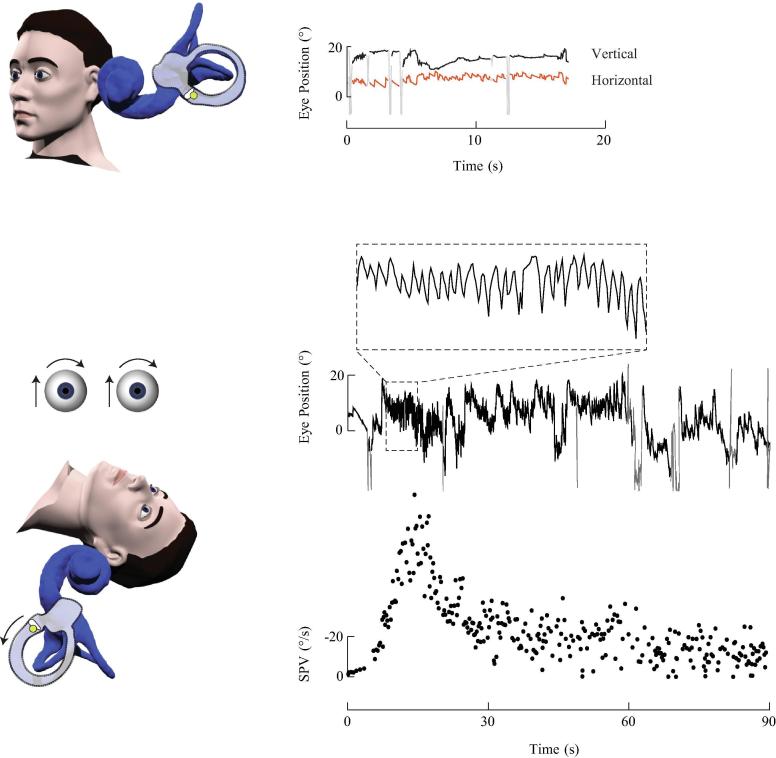
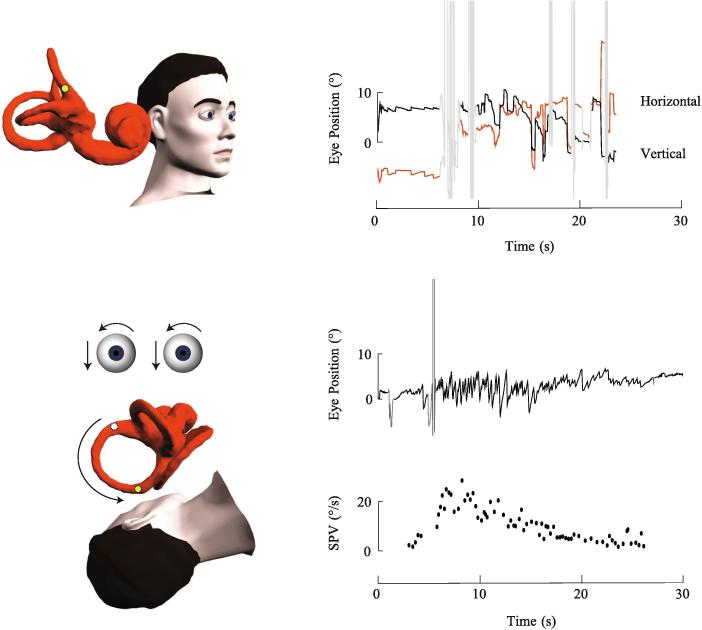
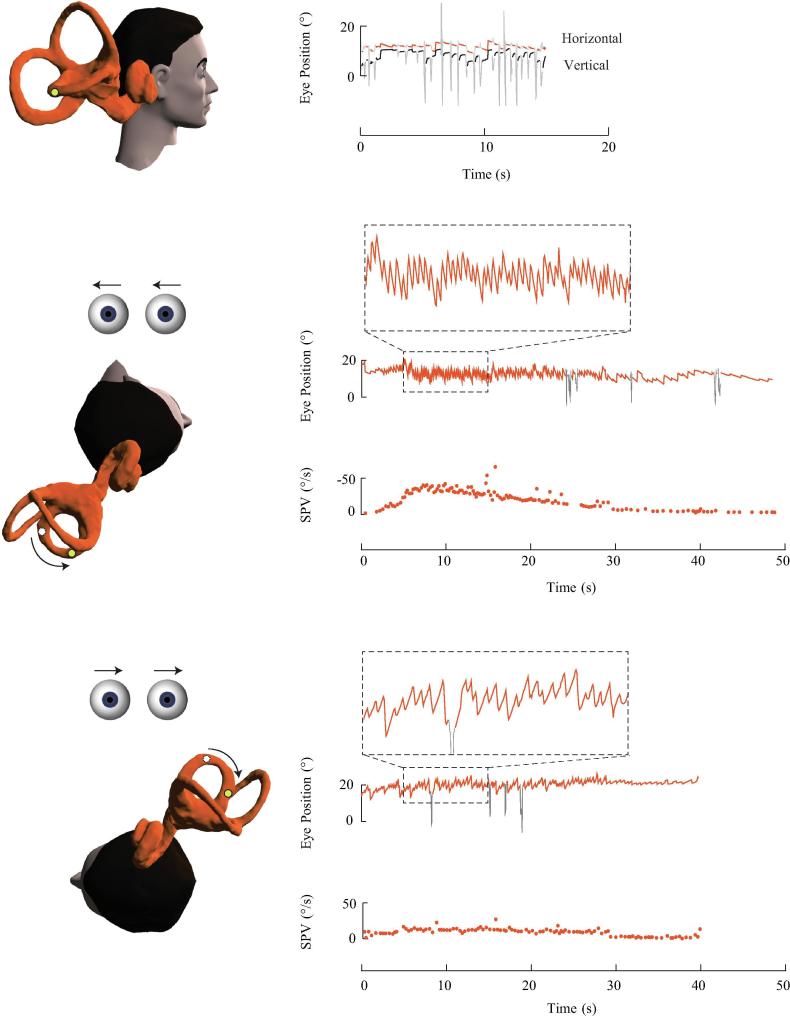
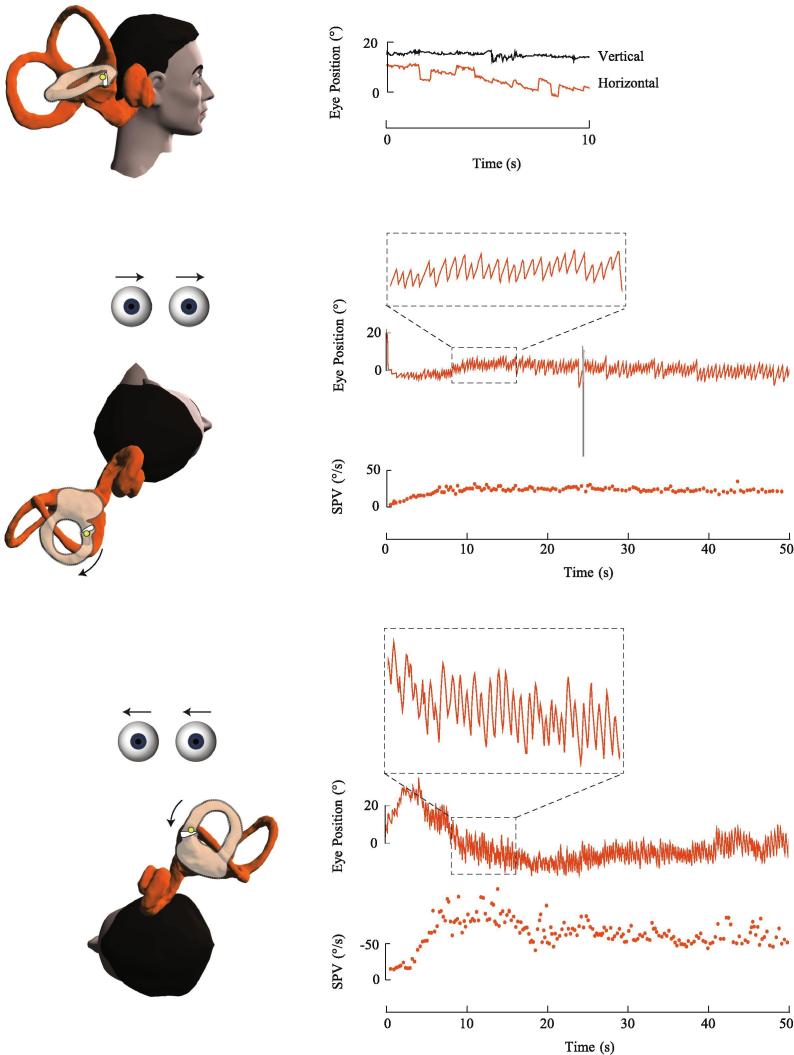
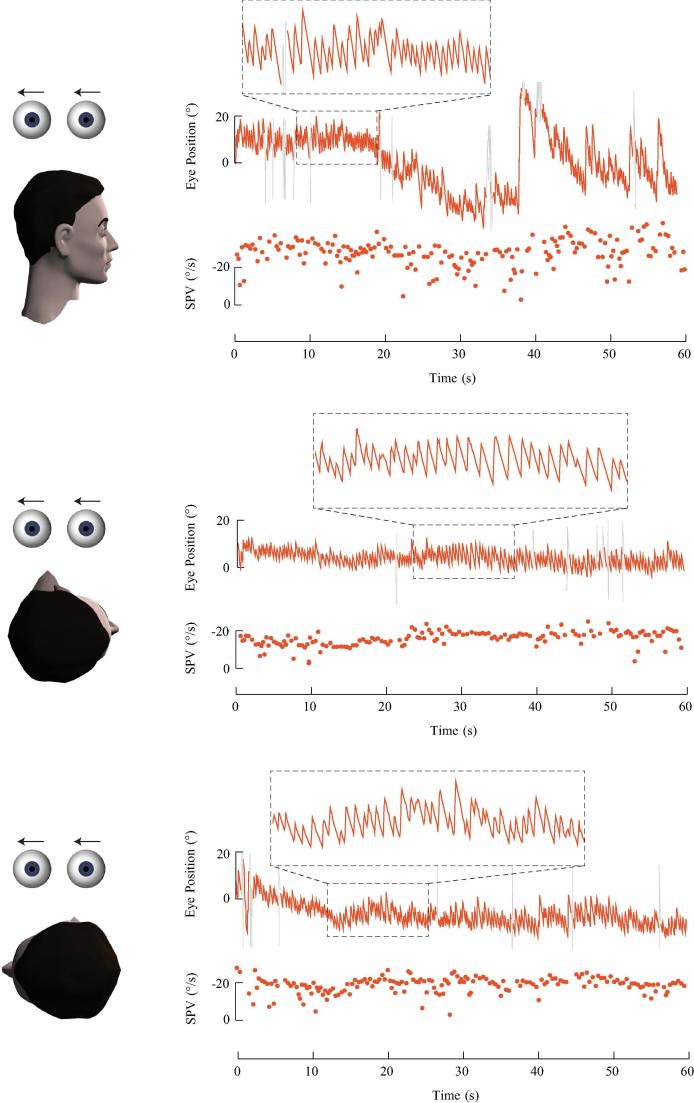
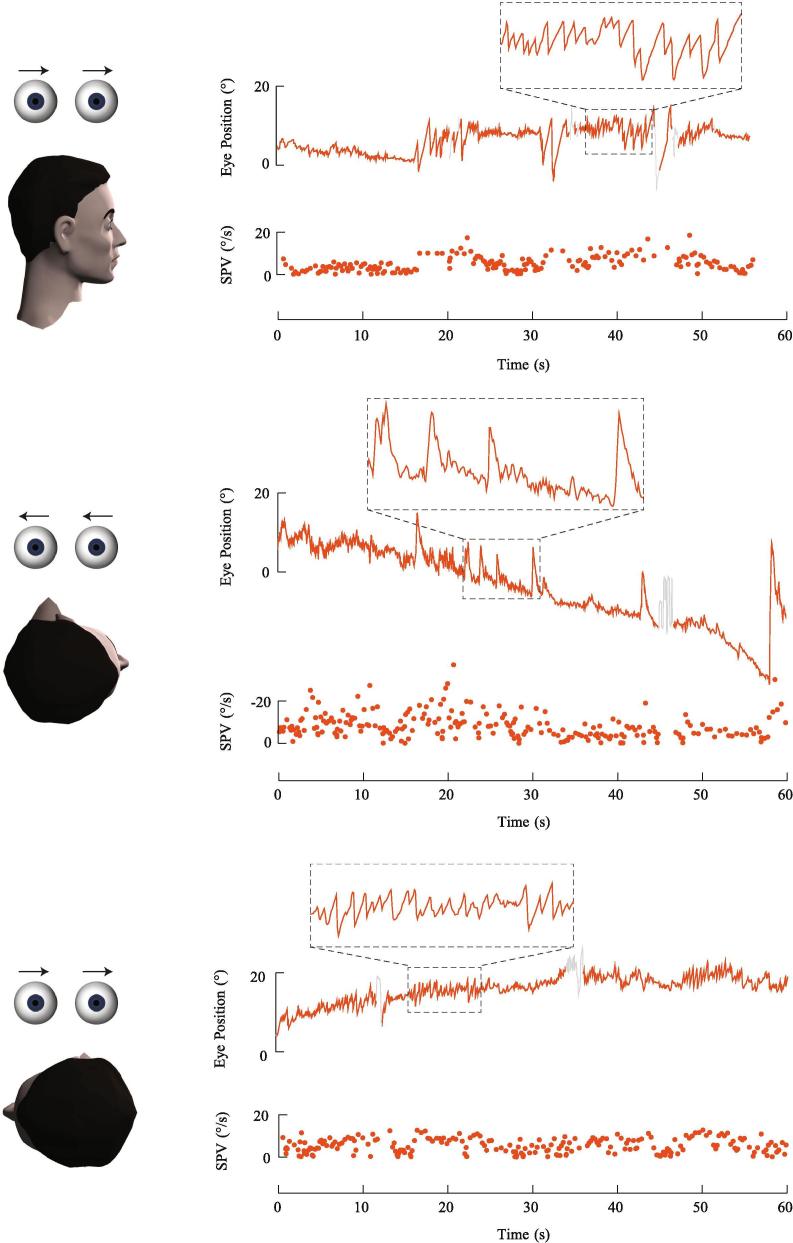
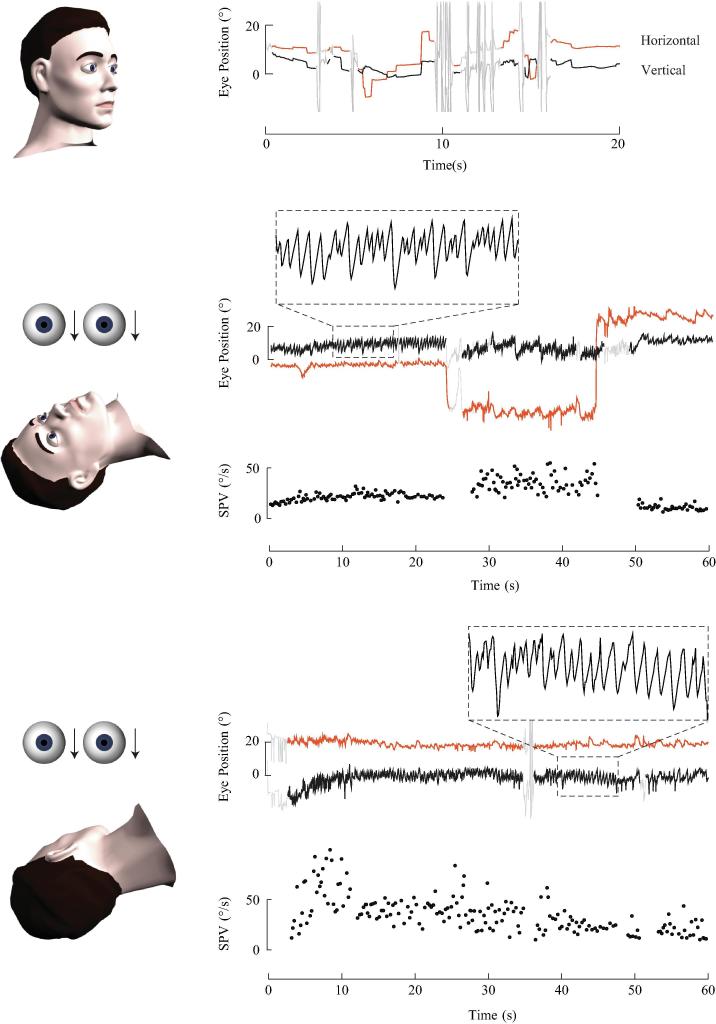
The diagnosis of benign positional vertigo (BPV) relies on a history of episodic positional vertigo and a distinctive pattern of nystagmus during provocative positional testing. The direction of the induced nystagmus is specific to the affected canal and the velocity profile reflects the underlying mechanism of canalithiasis (free-floating otoconia within the canal duct) or cupulolithiasis (otoconia adherent to the cupula). We review current theories on the pathophysiology of BPV, the clinical history and examination underlying its diagnosis, and recommended repositioning manoeuvres for each of the BPV subtypes. Disorders other than BPV which may present with a similar history and/or positional nystagmus are discussed.
Keywords: Benign paroxysmal positional vertigo; Canalithiasis; Cupulolithiasis; Positional nystagmus.
Figures
Similar articles
-
Cupulolithiasis: A Critical Reappraisal.OTO Open. 2023 Mar 1;7(1):e38. doi: 10.1002/oto2.38. eCollection 2023 Jan-Mar. OTO Open. 2023. PMID: 36998555 Free PMC article.
-
Practical neurology--4: Dizziness on head movement.Med J Aust. 2011 Nov 7;195(9):518-22. doi: 10.5694/mja11.11001. Med J Aust. 2011. PMID: 22060084
-
[Benign paroxysmal positional vertigo : Typical and unusual clinical findings].Nervenarzt. 2021 Aug;92(8):819-836. doi: 10.1007/s00115-021-01163-4. Epub 2021 Aug 2. Nervenarzt. 2021. PMID: 34338803 German.
-
Benign paroxysmal positional vertigo.Auris Nasus Larynx. 2022 Oct;49(5):737-747. doi: 10.1016/j.anl.2022.03.012. Epub 2022 Apr 3. Auris Nasus Larynx. 2022. PMID: 35387740 Review.
-
Classification, diagnostic criteria and management of benign paroxysmal positional vertigo.Auris Nasus Larynx. 2017 Feb;44(1):1-6. doi: 10.1016/j.anl.2016.03.013. Epub 2016 May 9. Auris Nasus Larynx. 2017. PMID: 27174206 Review.
Cited by
-
BPPV Simulation: A Powerful Tool to Understand and Optimize the Diagnostics and Treatment of all Possible Variants of BPPV.Front Neurol. 2021 Mar 26;12:632286. doi: 10.3389/fneur.2021.632286. eCollection 2021. Front Neurol. 2021. PMID: 33841305 Free PMC article.
-
A novel maneuver for diagnosis and treatment of torsional-vertical down beating positioning nystagmus: anterior canal and apogeotropic posterior canal BPPV.Braz J Otorhinolaryngol. 2022 Sep-Oct;88(5):708-716. doi: 10.1016/j.bjorl.2020.09.009. Epub 2020 Oct 28. Braz J Otorhinolaryngol. 2022. PMID: 33176986 Free PMC article.
-
Sequencing and Integration of Cervical Manual Therapy and Vestibulo-oculomotor Therapy for Concussion Symptoms: Retrospective Analysis.Int J Sports Phys Ther. 2021 Feb 1;16(1):12-20. doi: 10.26603/001c.18825. Int J Sports Phys Ther. 2021. PMID: 33604130 Free PMC article.
-
Apogeotropic Horizontal Canal Benign Paroxysmal Positional Vertigo: Zuma e Maia Maneuver versus Appiani Variant of Gufoni.Audiol Res. 2022 Jun 19;12(3):337-346. doi: 10.3390/audiolres12030035. Audiol Res. 2022. PMID: 35735368 Free PMC article.
-
The Implementation of a Return-to-Play Protocol with Standardized Physical Therapy Referrals in a Collegiate Football Program: PT's Role in Return-to-Play, A Clinical Commentary.Int J Sports Phys Ther. 2023 Apr 1;18(2):513-525. doi: 10.26603/001c.73074. eCollection 2023. Int J Sports Phys Ther. 2023. PMID: 37020444 Free PMC article.
References
-
- Ahmed R., Pohl D., MacDougall H., Makeham T., Halmagyi G. Posterior semicircular canal occlusion for intractable benign positional vertigo: outcome in 55 ears in 53 patients operated upon over 20 years. J. Laryngol. Otol. 2012;126(7):677–682. - PubMed
-
- Appiani G.C., Catania G., Gagliardi M., Cuiuli G. Repositioning maneuver for the treatment of the apogeotropic variant of horizontal canal benign paroxysmal positional vertigo. Otol. Neurotol. 2005;26(2):257–260. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
