

Application of ultrasound accelerates the decalcification process of bone matrix without affecting histological and immunohistochemical analysis
- PMID: 31194084
- PMCID: PMC6551353
- DOI: 10.1016/j.jot.2018.08.001
Application of ultrasound accelerates the decalcification process of bone matrix without affecting histological and immunohistochemical analysis
Abstract
Background/objectives: Decalcification of bone specimens is necessary for routine paraffin embedding and sectioning. Ethylenediaminetetraacetic acid (EDTA), a chelating agent for decalcification, maintains bone tissue integrity and histological features but requires long decalcification period, especially for cortical bone with dense mineral matrix. We hypothesised that the application of a newly commercially available ultrasound (US) decalcifier would accelerate decalcification of thick cortical bone specimen in EDTA efficiently and that the working temperature at 30-45°C would not affect histological and immunohistochemical analysis. Comparison was made with traditional decalcification method with regards to quality of tissue morphology and antigenicity.
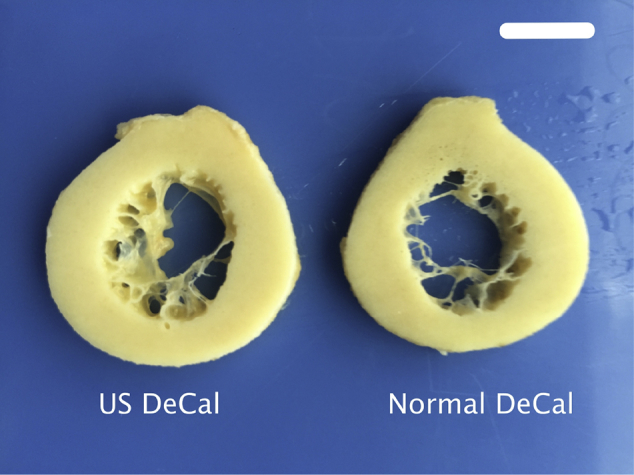
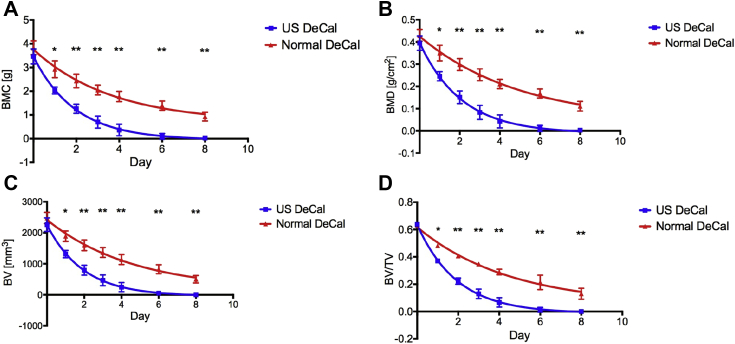
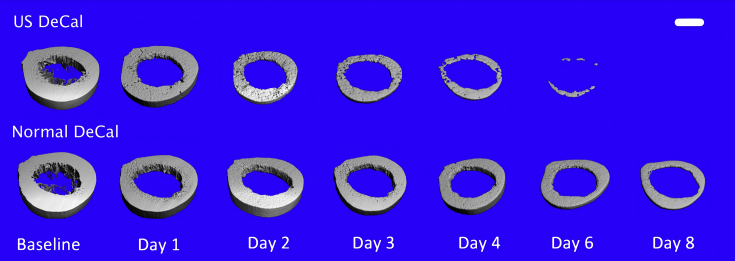
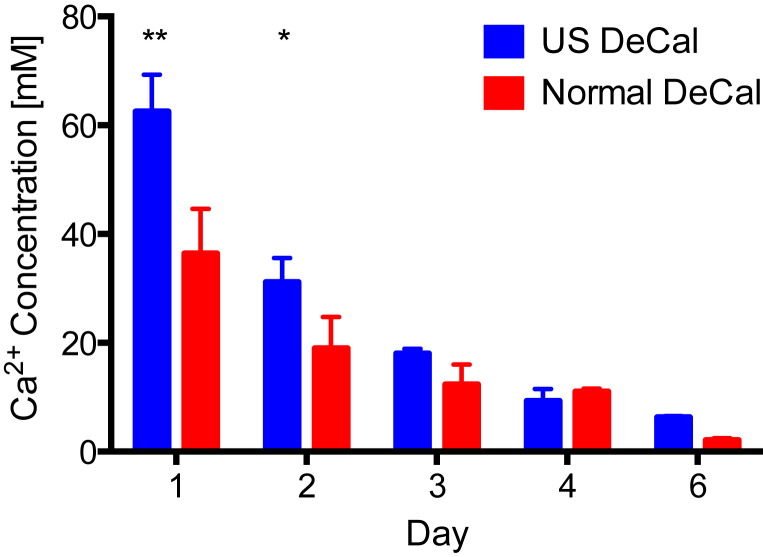
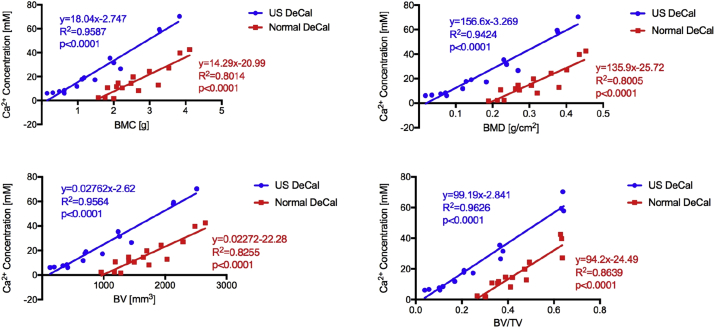
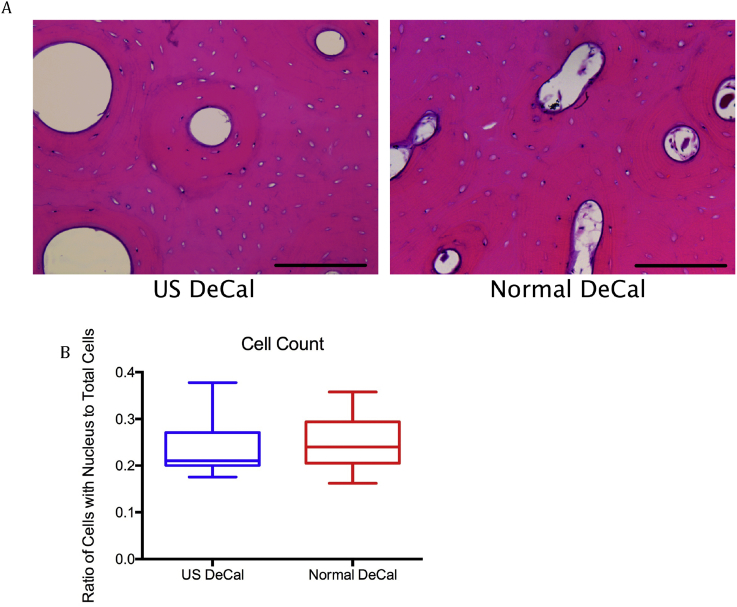
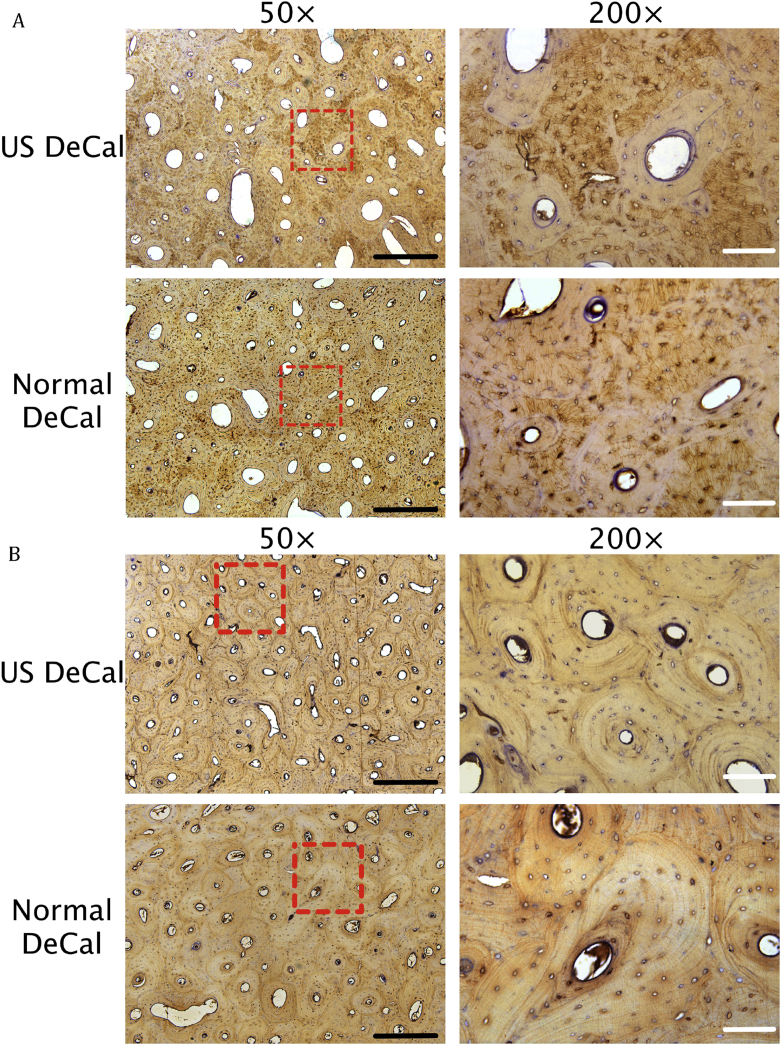
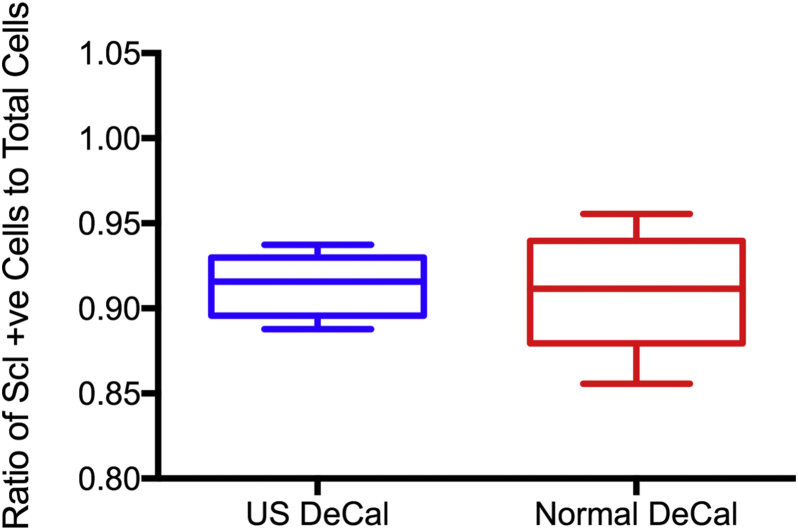
Methods: A fresh human cadaveric femoral shaft was sectioned into 5-mm-thick transverse sections. After fixation, the bone slices were divided into two groups: Ultrasound decalcification group (US DeCal), in which bone sections (n = 3) were placed in a US decalcifier (50 W at a frequency of 40kHz) with EDTA solution, and normal decalcification group (Normal DeCal), in which bone sections (n = 3) were decalcified in EDTA without US. The mineral content of the bone sections was measured with micro-computed tomography and dual-energy X-ray absorptiometry at different time points. Rate of calcium extraction was quantified by measuring the calcium concentration in EDTA solution using inductively coupled plasma optical emission spectrometry. After decalcification, the paraffin sections of the decalcified bone were stained with haematoxylin and eosin or immunohistochemical staining of sclerostin.
Results: Samples in US DeCal contained 2.9 ± 2.8% of the mineral content at Day 6 and were completely decalcified at Day 8. However, sections in Normal DeCal retained 36.3 ± 5.1% and 24.3 ± 4.8% at Day 6 and Day 8, respectively, and took six times longer to complete decalcification. The concentration of calcium in the EDTA solution of the US DeCal group was 70% higher than that of the Normal DeCal group (p < 0.05) in Day 1 and 2. No staining difference was observed in histological sections between the two groups.
Conclusion: The application of US decalcification significantly shortened the decalcification time in EDTA without causing histological artefacts.
The translational potential of this article: This article shows that the application of ultrasound in sample decalcification would shorten the duration that decalcification required. This would accelerate the sample processing for routine bone histology in both basic and clinical research and assessments for diagnostic purposes.
Keywords: Bone histology; Bone histomorphometry; Decalcification; Immunohistochemistry; Ultrasound.
Figures
Similar articles
-
Optimization of decalcification techniques for histologic examination of the rat maxillary and mandibular incisors for toxicity studies.J Histotechnol. 2022 Mar;45(1):2-9. doi: 10.1080/01478885.2021.1974780. Epub 2021 Sep 24. J Histotechnol. 2022. PMID: 34556002
-
A comparison of three decalcification agents for assessments of cranial fracture histomorphology.J Forensic Sci. 2022 May;67(3):1157-1166. doi: 10.1111/1556-4029.14990. Epub 2022 Feb 2. J Forensic Sci. 2022. PMID: 35112350
-
Advantages of a combined method of decalcification compared to EDTA.Microsc Res Tech. 2015 Feb;78(2):111-8. doi: 10.1002/jemt.22451. Epub 2014 Nov 28. Microsc Res Tech. 2015. PMID: 25452153
-
[Histological processing of iliac crest biopsies based on decalcification and paraffin embedding with reference to osteolytic and hematologic diagnosis].Pathologe. 1995 Jan;16(1):11-27. doi: 10.1007/s002920050071. Pathologe. 1995. PMID: 7886010 Review. German.
-
Resolving the bone - optimizing decalcification in spatial transcriptomics and molecular pathology.J Histotechnol. 2025 Mar;48(1):68-77. doi: 10.1080/01478885.2024.2446038. Epub 2024 Dec 26. J Histotechnol. 2025. PMID: 39723974 Review.
Cited by
-
Effects of fixation and demineralization on histomorphology and DNA amplification of canine bone marrow.Vet Pathol. 2024 Nov;61(6):943-951. doi: 10.1177/03009858241257920. Epub 2024 Jun 6. Vet Pathol. 2024. PMID: 38842072 Free PMC article.
-
Interleukin-19 promotes bone resorption by suppressing osteoprotegerin expression in BMSCs in a lipopolysaccharide-induced bone loss mouse model.Bone Joint Res. 2023 Nov 3;12(11):691-701. doi: 10.1302/2046-3758.1211.BJR-2023-0101.R1. Bone Joint Res. 2023. PMID: 37918438 Free PMC article.
-
Magnesium and vitamin C supplementation attenuates steroid-associated osteonecrosis in a rat model.Biomaterials. 2020 Apr;238:119828. doi: 10.1016/j.biomaterials.2020.119828. Epub 2020 Jan 31. Biomaterials. 2020. PMID: 32045781 Free PMC article.
-
Magnesium implantation or supplementation ameliorates bone disorder in CFTR-mutant mice through an ATF4-dependent Wnt/β-catenin signaling.Bioact Mater. 2021 Jul 3;8:95-108. doi: 10.1016/j.bioactmat.2021.06.034. eCollection 2022 Feb. Bioact Mater. 2021. PMID: 34541389 Free PMC article.
-
Hypertonic saline- and detergent-accelerated EDTA-based decalcification better preserves mRNA of bones.Sci Rep. 2024 May 13;14(1):10888. doi: 10.1038/s41598-024-61459-8. Sci Rep. 2024. PMID: 38740835 Free PMC article.
References
-
- Einhorn T.A., Simon S.R. 2nd ed. American Academy of Orthopaedic Surgeons; Rosemont, Ill: 2000. American Academy of Orthopaedic Surgeons. Orthopaedic basic science : biology and biomechanics of the musculoskeletal system.
-
- An Y.H., Martin K.L. Humana Press; Totowa, NJ: 2003. Handbook of histology methods for bone and cartilage.
-
- Kirita T. Springer Science+Business Media; New York, NY: 2015. Oral cancer.
-
- Prasad P., Donoghue M. A comparative study of various decalcification techniques. Indian J Dent Res. 2013;24(3):302–308. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
