

Prognostic Case Volume Thresholds in Patients With Head and Neck Squamous Cell Carcinoma
- PMID: 31194229
- PMCID: PMC6567848
- DOI: 10.1001/jamaoto.2019.1187
Prognostic Case Volume Thresholds in Patients With Head and Neck Squamous Cell Carcinoma
Abstract
Importance: Though described as an important prognostic indicator, facility case volume thresholds for patients with head and neck squamous cell carcinoma (HNSCC) have not been previously developed to date.
Objective: To identify prognostic case volume thresholds of facilities that manage HNSCC.
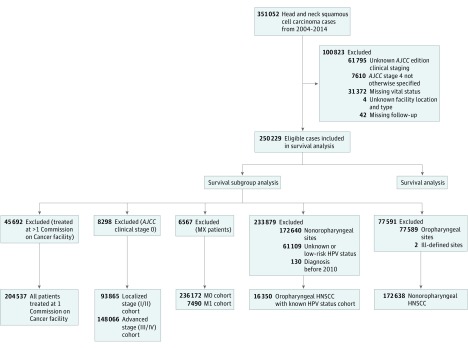
Design, setting, and participants: Retrospective analysis of 351 052 HNSCC cases reported from January 1, 2004, through December 31, 2014, by Commission of Cancer-accredited cancer centers from the US National Cancer Database. Data were analyzed from August 1, 2018, to April 5, 2019.
Exposures: Treatment of HNSCC at facilities with varying case volumes.
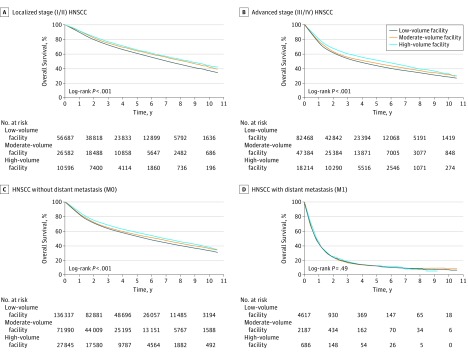
Main outcomes and measures: Using all-cause mortality outcomes among adult patients with HNSCC, 10 groups with increasing facility case volume were created and thresholds were identified where group survival differed compared with each of the 2 preceding groups (univariate log-rank analysis). Groups were collapsed at these thresholds and the prognostic value was confirmed using multivariable Cox regression. Prognostic meaning of these thresholds was assessed in subgroups by category (localized [I/II] and advanced [III/IV]), without metastasis (M0), with metastasis (M1), and anatomic subsites (nonoropharyngeal HNSCC and oropharyngeal HNSCC with known human papillomavirus status).
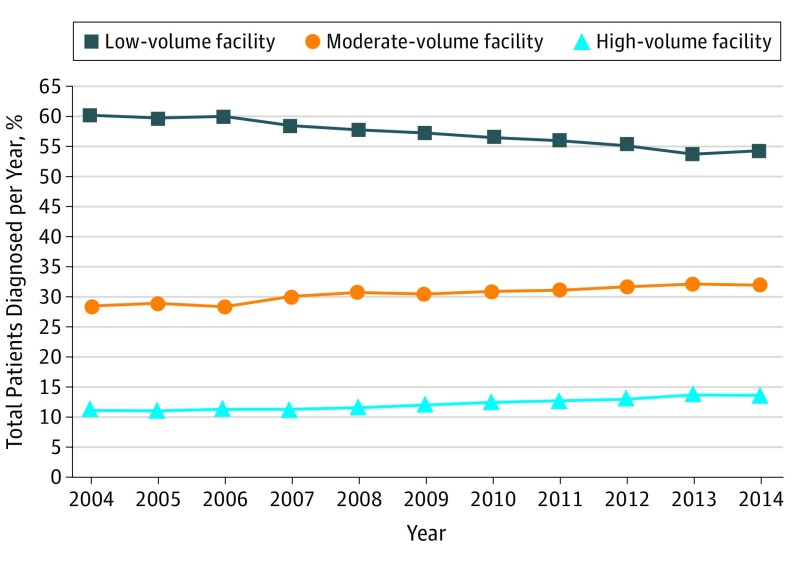
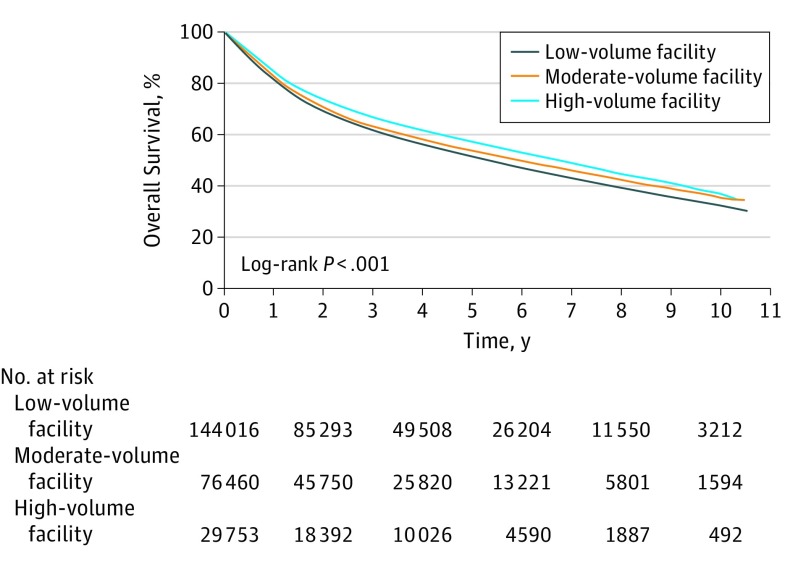
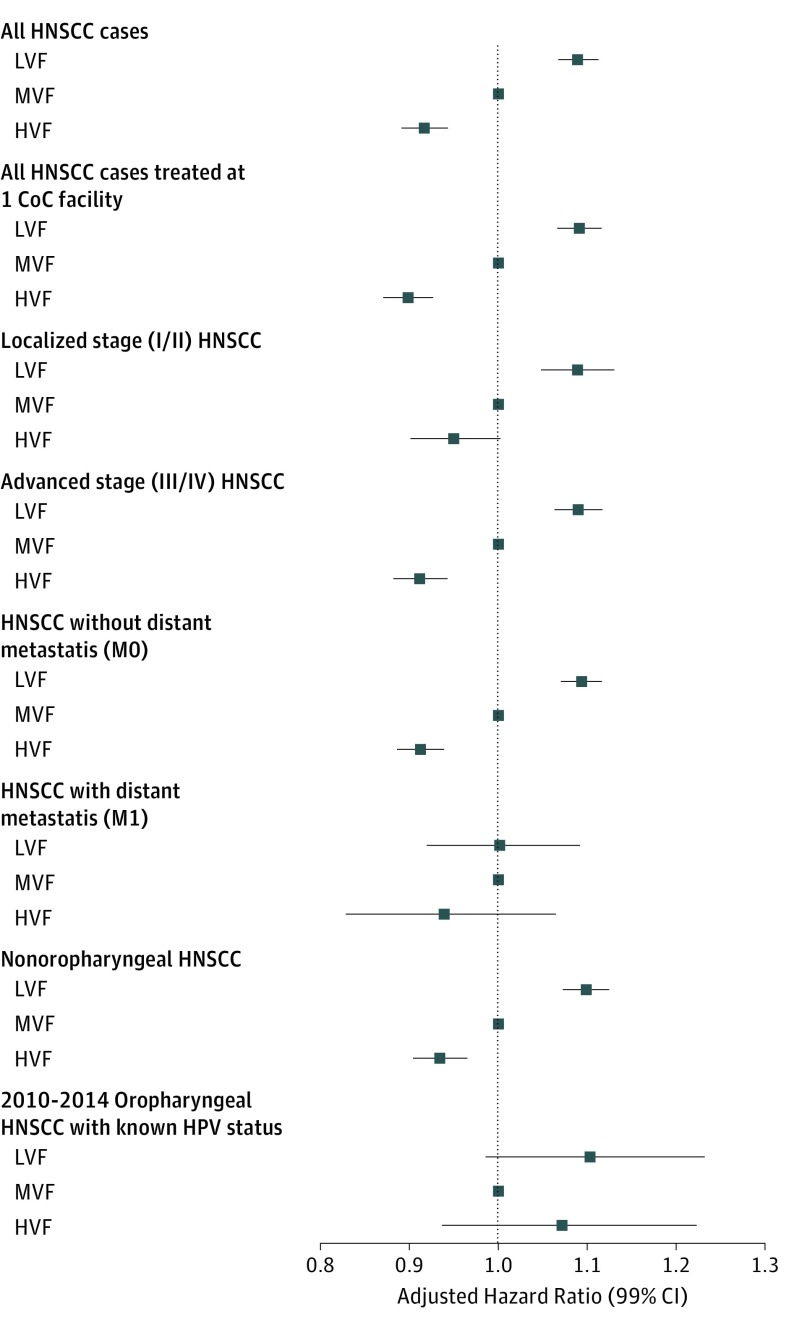
Results: Of 250 229 eligible patients treated at 1229 facilities in the United States, there were 185 316 (74.1%) men and 64 913 (25.9%) women and the mean (SD) age was 62.8 (12.1) years. Three case volume thresholds were identified (low: ≤54 cases per year; moderate: >54 to ≤165 cases per year; and high: >165 cases per year). Compared with the moderate-volume group, multivariate analysis found that treatment at low-volume facilities (LVFs) was associated with a higher risk of mortality (hazard ratio [HR], 1.09; 99% CI, 1.07-1.11), whereas treatment at high-volume facilities (HVFs) was associated with a lower risk of mortality (HR, 0.92; 99% CI, 0.89-0.94). Subgroup analysis with Bonferroni correction revealed that only the moderate- vs low- threshold had meaningful differences in outcomes in localized stage (I/II) cancers, (LVFs vs moderate-volume facilities [MVFs]: HR, 1.09 [99% CI, 1.05-1.13]; HVF vs MVF: HR, 0.95 [99% CI, 0.90-1.00]), whereas both thresholds were meaningful in advanced stage (III/IV) cancers (LVF vs MVF: HR, 1.09 [99% CI, 1.06-1.12]; HVF vs MVF: HR, 0.91 [99% CI, 0.88-0.94]). Survival differed by prognostic thresholds for both M0 (LVF vs MVF: HR, 1.09 [99% CI, 1.07-1.12]; HVF vs MVF: HR, 0.91 [99% CI, 0.89-0.94]) and nonoropharyngeal HNSCC (LVF vs MVF: HR, 1.10 [99% CI, 1.07-1.13]; HVF vs MVF: HR, 0.93 [99% CI, 0.90-0.97]) site cases, but not for M1 (LVF vs MVF: HR, 1.00 [99% CI, 0.92-1.09]; HVF vs MVF: HR, 0.94 [99% CI, 0.83-1.07]) or oropharyngeal HNSCC cases (when controlling for human papillomavirus status) (LVF vs MVF: HR, 1.10 [99% CI, 0.99-1.23]; HVF vs MVF: HR, 1.07 [99% CI, 0.94-1.22]).
Conclusions and relevance: Higher volume facility threshold results appear to be associated with increases in survival rates for patients treated for HNSCC at MVFs or HVFs compared with LVFs, which suggests that these thresholds may be used as quality markers.
Conflict of interest statement
Figures
Similar articles
-
Treatment at high-volume facilities and academic centers is independently associated with improved survival in patients with locally advanced head and neck cancer.Cancer. 2017 Oct 15;123(20):3933-3942. doi: 10.1002/cncr.30843. Epub 2017 Jun 22. Cancer. 2017. PMID: 28640546
-
Facility Volume and Changing Facilities for Postoperative Radiotherapy in Salivary Gland Cancer.Laryngoscope. 2024 Dec;134(12):4935-4946. doi: 10.1002/lary.31588. Epub 2024 Jun 19. Laryngoscope. 2024. PMID: 38895869
-
Facility Volume as a Prognosticator of Survival in Locally Advanced Papillary Thyroid Cancer.Laryngoscope. 2023 Feb;133(2):443-450. doi: 10.1002/lary.30280. Epub 2022 Jul 13. Laryngoscope. 2023. PMID: 35822421 Free PMC article.
-
Impact of facility type and volume in low-grade glioma outcomes.J Neurosurg. 2019 Sep 27;133(5):1313-1323. doi: 10.3171/2019.6.JNS19409. Print 2020 Nov 1. J Neurosurg. 2019. PMID: 31561219
-
The prognostic role of PD-L1 expression for survival in head and neck squamous cell carcinoma: A systematic review and meta-analysis.Oral Oncol. 2018 Nov;86:81-90. doi: 10.1016/j.oraloncology.2018.09.016. Epub 2018 Sep 17. Oral Oncol. 2018. PMID: 30409325
Cited by
-
Quality of Life, Toxicity and Unmet Needs in Nasopharyngeal Cancer Survivors.Front Oncol. 2020 Jun 12;10:930. doi: 10.3389/fonc.2020.00930. eCollection 2020. Front Oncol. 2020. PMID: 32596155 Free PMC article. Review.
-
Vascular Endothelial Growth Factor: A Translational View in Oral Non-Communicable Diseases.Biomolecules. 2021 Jan 12;11(1):85. doi: 10.3390/biom11010085. Biomolecules. 2021. PMID: 33445558 Free PMC article. Review.
-
Implementing a virtual multidisciplinary clinical case discussion to manage rare and complex head and neck cancers: an expert-defined protocol proposal from the Italian Association of Head and Neck Oncology (AIOCC).Acta Otorhinolaryngol Ital. 2023 Feb;43(1):82-84. doi: 10.14639/0392-100X-N2368. Acta Otorhinolaryngol Ital. 2023. PMID: 36860154 Free PMC article.
-
Volume Outcome Relationships of Oropharyngeal Cancer Patients Undergoing Transoral Robotic Surgery.Laryngoscope. 2025 Aug;135(8):2810-2818. doi: 10.1002/lary.32098. Epub 2025 Mar 3. Laryngoscope. 2025. PMID: 40026255 Free PMC article.
-
Multidisciplinary survey on use of feeding tubes in head and neck cancer patients undergoing chemoradiotherapy in Germany-the SUFEETUBE project.Strahlenther Onkol. 2024 Jul;200(7):583-594. doi: 10.1007/s00066-024-02206-w. Epub 2024 Feb 21. Strahlenther Onkol. 2024. PMID: 38381142 Free PMC article.
References
-
- National Comprehensive Cancer Network (NCCN) NCCN Clinical Practice Guidelines in Oncology. Head and Neck Cancers, version 2. 2018. National Comprehensive Cancer Network. http://oncolife.com.ua/doc/nccn/Head_and_Neck_Cancers.pdf Accessed May 12, 2019. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
