

Antibodies against ARHGDIB are associated with long-term kidney graft loss
- PMID: 31194283
- PMCID: PMC6899679
- DOI: 10.1111/ajt.15493
Antibodies against ARHGDIB are associated with long-term kidney graft loss
Abstract
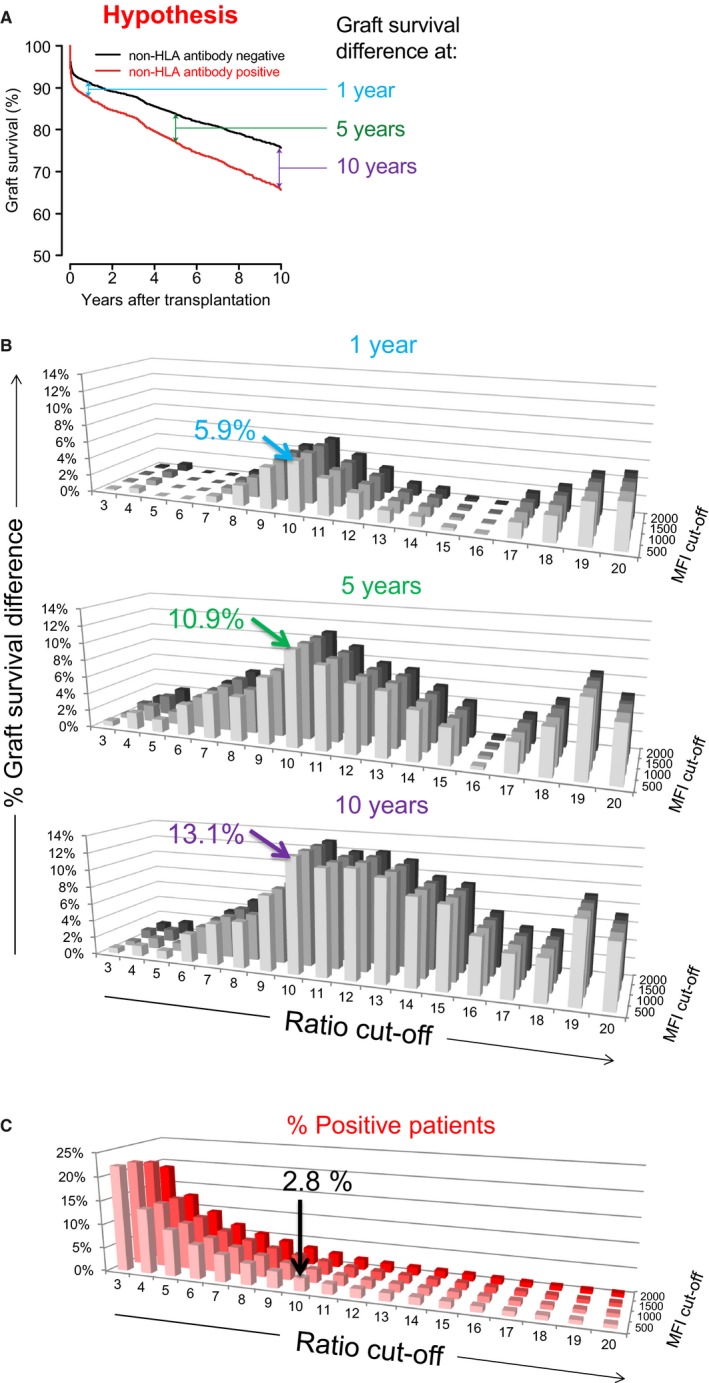
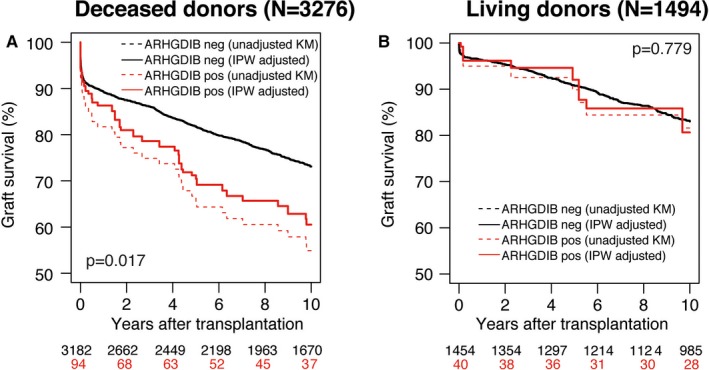
The clinical significance of non-HLA antibodies on renal allograft survival is a matter of debate, due to differences in reported results and lack of large-scale studies incorporating analysis of multiple non-HLA antibodies simultaneously. We developed a multiplex non-HLA antibody assay against 14 proteins highly expressed in the kidney. In this study, the presence of pretransplant non-HLA antibodies was correlated to renal allograft survival in a nationwide cohort of 4770 recipients transplanted between 1995 and 2006. Autoantibodies against Rho GDP-dissociation inhibitor 2 (ARHGDIB) were significantly associated with graft loss in recipients transplanted with a deceased-donor kidney (N = 3276) but not in recipients of a living-donor kidney (N = 1496). At 10 years after deceased-donor transplantation, recipients with anti-ARHGDIB antibodies (94/3276 = 2.9%) had a 13% lower death-censored covariate-adjusted graft survival compared to the anti-ARHGDIB-negative (3182/3276 = 97.1%) population (hazard ratio 1.82; 95% confidence interval, 1.32-2.53; P = .0003). These antibodies occur independently from donor-specific anti-HLA antibodies (DSA) or other non-HLA antibodies investigated. No significant relations with graft loss were found for the other 13 non-HLA antibodies. We suggest that pretransplant risk assessment can be improved by measuring anti-ARHGDIB antibodies in all patients awaiting deceased-donor transplantation.
Keywords: ARHGDIB; kidney transplantation; non-HLA antibodies.
© 2019 The Authors. American Journal of Transplantation published by Wiley Periodicals, Inc. on behalf of The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures
References
-
- World Kidney Day . Chronic kidney disease. 2018. https://www.worldkidneyday.org/faqs/chronic-kidney-disease. Accessed September 12, 2018.
-
- Tait BD, Süsal C, Gebel HM, et al. Consensus guidelines on the testing and clinical management issues associated with HLA and non‐HLA antibodies in transplantation. Transplantation. 2013;95(1):19‐47. - PubMed
-
- Deltombe C, Gillaizeau F, Anglicheau D, et al. Is pre‐transplant sensitization against angiotensin II type 1 receptor still a risk factor of graft and patient outcome in kidney transplantation in the anti‐HLA Luminex era? A retrospective study Transpl Int. 2017;30(11):1150‐1160. - PubMed
-
- Giral M, Foucher Y, Dufay A, et al. Pretransplant sensitization against angiotensin II type 1 receptor is a risk factor for acute rejection and graft loss. Am J Transplant. 2013;13(10):2567‐2576. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
