

Can clinical prediction models assess antibiotic need in childhood pneumonia? A validation study in paediatric emergency care
- PMID: 31194750
- PMCID: PMC6563975
- DOI: 10.1371/journal.pone.0217570
Can clinical prediction models assess antibiotic need in childhood pneumonia? A validation study in paediatric emergency care
Abstract
Objectives: Pneumonia is the most common bacterial infection in children at the emergency department (ED). Clinical prediction models for childhood pneumonia have been developed (using chest x-ray as their reference standard), but without implementation in clinical practice. Given current insights in the diagnostic limitations of chest x-ray, this study aims to validate these prediction models for a clinical diagnosis of pneumonia, and to explore their potential to guide decisions on antibiotic treatment at the ED.
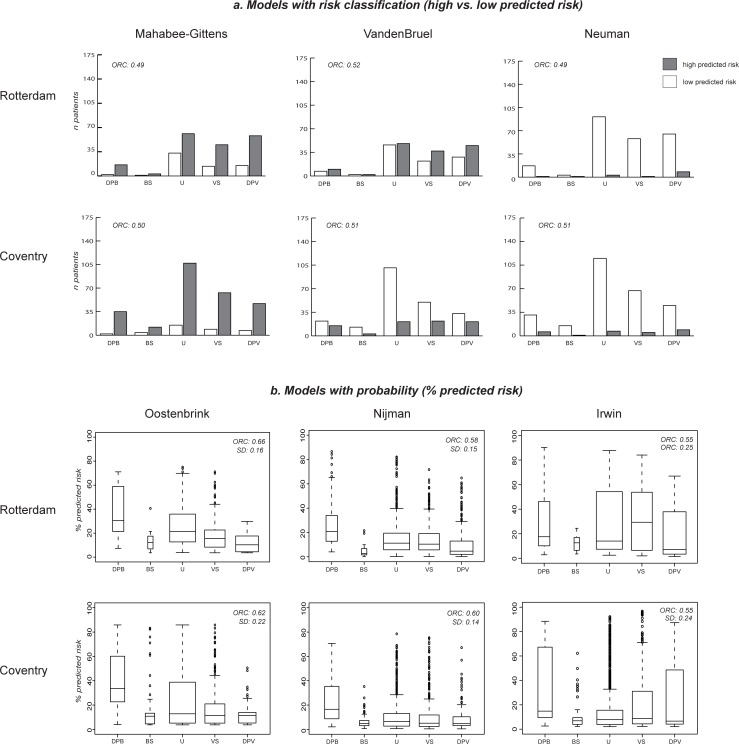
Methods: We systematically identified clinical prediction models for childhood pneumonia and assessed their quality. We evaluated the validity of these models in two populations, using a clinical reference standard (1. definite/probable bacterial, 2. bacterial syndrome, 3. unknown bacterial/viral, 4. viral syndrome, 5. definite/probable viral), measuring performance by the ordinal c-statistic (ORC). Validation populations included prospectively collected data of children aged 1 month to 5 years attending the ED of Rotterdam (2012-2013) or Coventry (2005-2006) with fever and cough or dyspnoea.
Results: We identified eight prediction models and could evaluate the validity of seven, with original good performance. In the Dutch population 22/248 (9%) had a bacterial infection, in Coventry 53/301 (17%), antibiotic prescription was 21% and 35% respectively. Three models predicted a higher risk in children with bacterial infections than in those with viral disease (ORC ≥0.55) and could identify children at low risk of bacterial infection.
Conclusions: Three clinical prediction models for childhood pneumonia could discriminate fairly well between a clinical reference standard of bacterial versus viral infection. However, they all require the measurement of biomarkers, raising questions on the exact target population when implementing these models in clinical practice. Moreover, choosing optimal thresholds to guide antibiotic prescription is challenging and requires careful consideration of potential harms and benefits.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Evaluation of a clinical decision rule to guide antibiotic prescription in children with suspected lower respiratory tract infection in The Netherlands: A stepped-wedge cluster randomised trial.PLoS Med. 2020 Jan 31;17(1):e1003034. doi: 10.1371/journal.pmed.1003034. eCollection 2020 Jan. PLoS Med. 2020. PMID: 32004317 Free PMC article. Clinical Trial.
-
Children with fever and cough at emergency care: diagnostic accuracy of a clinical model to identify children at low risk of pneumonia.Eur J Emerg Med. 2013 Aug;20(4):273-80. doi: 10.1097/MEJ.0b013e32835771fd. Eur J Emerg Med. 2013. PMID: 22868746
-
The influence of chest X-ray results on antibiotic prescription for childhood pneumonia in the emergency department.Eur J Pediatr. 2021 Sep;180(9):2765-2772. doi: 10.1007/s00431-021-03996-2. Epub 2021 Mar 22. Eur J Pediatr. 2021. PMID: 33754207 Free PMC article. Clinical Trial.
-
Clinical prediction models for young febrile infants at the emergency department: an international validation study.Arch Dis Child. 2018 Nov;103(11):1033-1041. doi: 10.1136/archdischild-2017-314011. Epub 2018 May 24. Arch Dis Child. 2018. PMID: 29794106
-
A systematic review of the clinical features of pneumonia in children aged 5-9 years: Implications for guidelines and research.J Glob Health. 2022 Mar 26;12:10002. doi: 10.7189/jogh.12.10002. eCollection 2022. J Glob Health. 2022. PMID: 35356655 Free PMC article.
Cited by
-
Risk prediction models to guide antibiotic prescribing: a study on adult patients with uncomplicated upper respiratory tract infections in an emergency department.Antimicrob Resist Infect Control. 2020 Nov 2;9(1):171. doi: 10.1186/s13756-020-00825-3. Antimicrob Resist Infect Control. 2020. PMID: 33138859 Free PMC article.
-
Predicting the causative pathogen among children with pneumonia using a causal Bayesian network.PLoS Comput Biol. 2023 Mar 13;19(3):e1010967. doi: 10.1371/journal.pcbi.1010967. eCollection 2023 Mar. PLoS Comput Biol. 2023. PMID: 36913404 Free PMC article.
-
Antimicrobial Stewardship in Pediatric Emergency Medicine: A Narrative Exploration of Antibiotic Overprescribing, Stewardship Interventions, and Performance Metrics.Children (Basel). 2024 Feb 23;11(3):276. doi: 10.3390/children11030276. Children (Basel). 2024. PMID: 38539311 Free PMC article. Review.
-
External validation of the RISC, RISC-Malawi, and PERCH clinical prediction rules to identify risk of death in children hospitalized with pneumonia.J Glob Health. 2021 Oct 9;11:04062. doi: 10.7189/jogh.11.04062. eCollection 2021. J Glob Health. 2021. PMID: 34737862 Free PMC article.
-
Evaluation of the impact of COVID-19 pandemic on hospital admission related to common infections: Risk prediction models to tackle antimicrobial resistance in primary care.PLoS One. 2024 Dec 31;19(12):e0311515. doi: 10.1371/journal.pone.0311515. eCollection 2024. PLoS One. 2024. PMID: 39739781 Free PMC article.
References
-
- Collaborators GBDLRI. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory infections in 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Infect Dis. 2018;18(11):1191–210. Epub 2018/09/24. [pii] 10.1016/S1473-3099(18)30310-4 - DOI - PMC - PubMed
-
- Harris M, Clark J, Coote N, Fletcher P, Harnden A, McKean M, et al. British Thoracic Society guidelines for the management of community acquired pneumonia in children: update 2011. Thorax. 2011;66 Suppl 2:ii1–23. Epub 2011/10/19. thoraxjnl-2011-200598 [pii] 10.1136/thoraxjnl-2011-200598 . - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
