

Spinal anesthesia for lumbar spine surgery correlates with fewer total medications and less frequent use of vasoactive agents: A single center experience
- PMID: 31194777
- PMCID: PMC6563985
- DOI: 10.1371/journal.pone.0217939
Spinal anesthesia for lumbar spine surgery correlates with fewer total medications and less frequent use of vasoactive agents: A single center experience
Abstract
Study objective: Anesthesiologists at our hospital commonly administer spinal anesthesia for routine lumbar spine surgeries. Anecdotal impressions suggested that patients received fewer anesthesia-administered intravenous medications, including vasopressors, during spinal versus general anesthesia. We hypothesized that data review would confirm these impressions. The objective was to test this hypothesis by comparing specific elements of spinal versus general anesthesia for 1-2 level open lumbar spine procedures.
Design: Retrospective single institutional study.
Setting: Academic medical center, operating rooms.
Patients: Consecutive patients (144 spinal and 619 general anesthesia) identified by automatic structured query of our electronic anesthesia record undergoing lumbar decompression, foraminotomy or microdiscectomy by one surgeon under general or spinal anesthesia.
Interventions: Spinal or general anesthesia.
Measurements: Numbers of medications administered during the case.
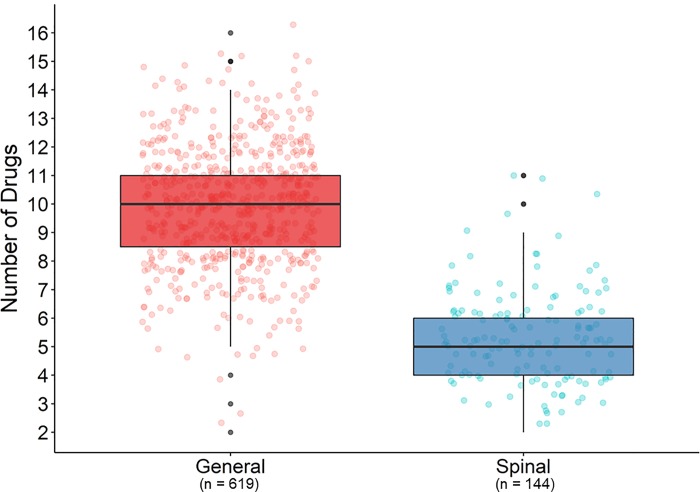
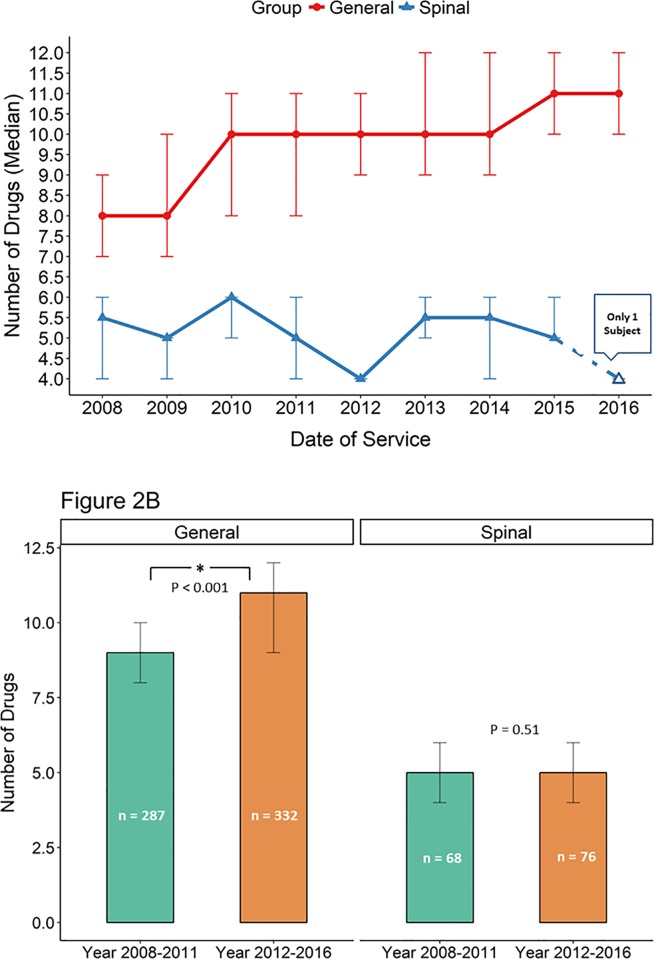
Main results: Anesthesiologists administered in the operating room a total of 10 ± 2 intravenous medications for general anesthetics and 5 ± 2 medications for spinal anesthetics (-5, 95% CI -5 to -4, p<0.001, univariate analysis). Multivariable analysis supported this finding (spinal versus general anesthesia: -4, 95% CI -5 to -4, p<0.001). Spinal anesthesia patients were less likely to receive ephedrine, or phenylephrine (by bolus or by infusion) (all p<0.001, Chi-squared test). Spinal anesthesia patients were also less likely to receive labetolol or esmolol (both p = 0.002, Fishers' Exact test). No neurologic injuries were attributed to, or masked by, spinal anesthesia. Three spinal anesthetics failed.
Conclusions: For routine lumbar surgery in our cohort, spinal compared to general anesthesia was associated with significantly fewer drugs administered during a case and less frequent use of vasoactive agents. Safety implications include greater hemodynamic stability with spinal anesthesia along with reduced risks for medication error and transmission of pathogens associated with medication administration.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Cost Analysis of Spinal Versus General Anesthesia for Lumbar Diskectomy and Laminectomy Spine Surgery.World Neurosurg. 2016 May;89:266-71. doi: 10.1016/j.wneu.2016.02.022. Epub 2016 Feb 11. World Neurosurg. 2016. PMID: 26875652
-
Spinal Anesthesia in Elderly Patients Undergoing Lumbar Spine Surgery.Orthopedics. 2017 Mar 1;40(2):e317-e322. doi: 10.3928/01477447-20161219-01. Epub 2016 Dec 28. Orthopedics. 2017. PMID: 28027388
-
Comparison of spinal and general anesthesia in lumbar laminectomy surgery: a case-controlled analysis of 400 patients.J Neurosurg Spine. 2005 Jan;2(1):17-22. doi: 10.3171/spi.2005.2.1.0017. J Neurosurg Spine. 2005. PMID: 15658121
-
Regional anesthesia versus general anesthesia for surgery on the lumbar spine: a review of the modern literature.Clin Neurol Neurosurg. 2014 Apr;119:39-43. doi: 10.1016/j.clineuro.2014.01.016. Epub 2014 Jan 27. Clin Neurol Neurosurg. 2014. PMID: 24635923 Review.
-
A Comparison of Regional Versus General Anesthesia for Lumbar Spine Surgery: A Meta-Analysis of Randomized Studies.J Neurosurg Anesthesiol. 2017 Oct;29(4):415-425. doi: 10.1097/ANA.0000000000000362. J Neurosurg Anesthesiol. 2017. PMID: 27564561 Review.
Cited by
-
Spinal Versus General Anesthesia for Lumbar Decompression or Sequestrectomy in Patients Over 75 Years.Clin Spine Surg. 2023 Aug 1;36(7):E329-E331. doi: 10.1097/BSD.0000000000001456. Epub 2023 Mar 31. Clin Spine Surg. 2023. PMID: 37012621 Free PMC article.
-
Comparative outcome analysis of spinal anesthesia versus general anesthesia in lumbar fusion surgery.J Clin Orthop Trauma. 2020 Nov 27;13:122-126. doi: 10.1016/j.jcot.2020.11.017. eCollection 2021 Feb. J Clin Orthop Trauma. 2020. PMID: 33680810 Free PMC article.
-
Spinal Versus General Anesthesia for Spine Surgery During the COVID-19 Pandemic: A Case Series.Anesth Pain Med. 2023 Mar 29;13(2):e134783. doi: 10.5812/aapm-134783. eCollection 2023 Apr. Anesth Pain Med. 2023. PMID: 37601956 Free PMC article.
-
A protocol for lumbar spine surgery under spinal anesthesia in resource limited countries: illustrative case series.Ann Med Surg (Lond). 2025 Jan 9;87(1):49-55. doi: 10.1097/MS9.0000000000002824. eCollection 2025 Jan. Ann Med Surg (Lond). 2025. PMID: 40109634 Free PMC article.
References
-
- Ditzler JW, Dumke PR, Harrington JJ, Fox JD. Should spinal anesthesia be used in surgery for herniated intervertebral disk. Anesth Analg. 1959;38(2):118–24. - PubMed
-
- Jellish WS, Thalji Z, Stevenson K, Shea J. A prospective randomized study comparing short- and intermediate-term perioperative outcome variables after spinal or general anesthesia for lumbar disk and laminectomy surgery. Anesth Analg. 1996;83(3):559–64. - PubMed
-
- Rung GW, Williams D, Gelb DE, Grubb M. Isobaric spinal anesthesia for lumbar disk surgery. Anesth Analg. 1997;84(5):1165–6. - PubMed
-
- Tetzlaff JE, Dilger JA, Kodsy M, al-Bataineh J, Yoon HJ, Bell GR. Spinal anesthesia for elective lumbar spine surgery. J Clin Anesth. 1998;10(8):666–9. - PubMed
-
- McLain RF, Bell GR, Kalfas I, Tetzlaff JE, Yoon HJ. Complications associated with lumbar laminectomy: a comparison of spinal versus general anesthesia. Spine (Phila Pa 1976). 2004;29(22):2542–7. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
