

Multimodal prehabilitation to reduce the incidence of delirium and other adverse events in elderly patients undergoing elective major abdominal surgery: An uncontrolled before-and-after study
- PMID: 31194798
- PMCID: PMC6564537
- DOI: 10.1371/journal.pone.0218152
Multimodal prehabilitation to reduce the incidence of delirium and other adverse events in elderly patients undergoing elective major abdominal surgery: An uncontrolled before-and-after study
Abstract
Background: Delirium is a common and serious complication in elderly patients undergoing major abdominal surgery, with significant adverse outcomes. Successful strategies or therapies to reduce the incidence of delirium are scarce. The objective of this study was to assess the role of prehabilitation in reducing the incidence of delirium in elderly patients.
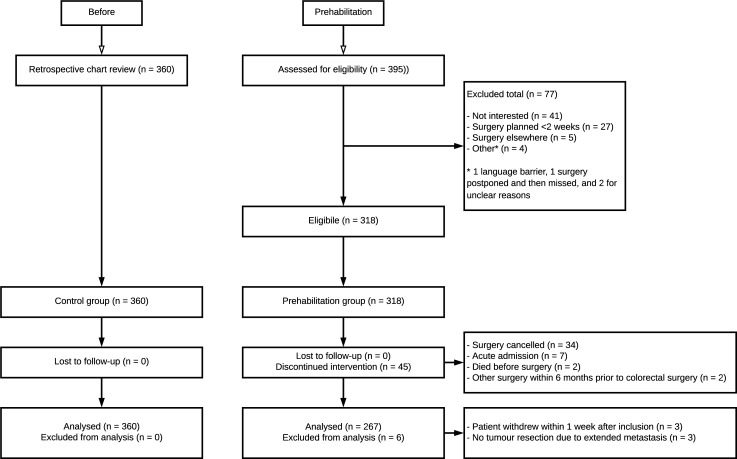
Methods: A single-center uncontrolled before-and-after study was conducted, including patients aged 70 years or older who underwent elective abdominal surgery for colorectal carcinoma or an abdominal aortic aneurysm between January 2013 and October 2015 (control group) and between November 2015 and June 2018 (prehabilitation group). The prehabilitation group received interventions to improve patients' physical health, nutritional status, factors of frailty and preoperative anaemia prior to surgery. The primary outcome was incidence of delirium, diagnosed with the DSM-V criteria or the confusion assessment method. Secondary outcomes were additional complications, length of stay, unplanned ICU admission, length of ICU stay, readmission rate, institutionalization, and in-hospital or 30-day mortality.
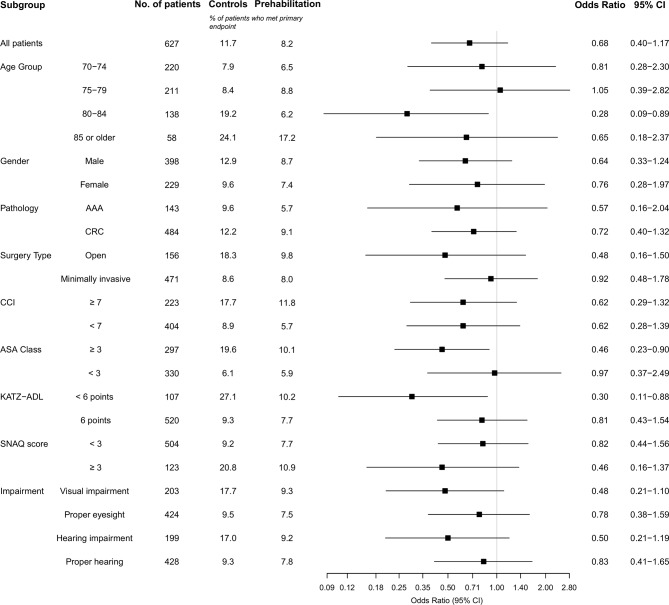
Result: A total of 360 control patients and 267 prehabilitation patients were included in the final analysis. The mean number of prehabilitation days was 39 days. The prehabilitation group had a higher burden of comorbidities and was more physically and visually impaired at baseline. At adjusted logistic regression analysis, delirium incidence was reduced significantly from 11.7 to 8.2% (OR 0.56; 95% CI 0.32-0.98; P = 0.043). No statistically significant effects were seen on secondary outcomes.
Conclusion: Current prehabilitation program is feasible and safe, and can reduce delirium incidence in elderly patients undergoing elective major abdominal surgery. This program merits further evaluation.
Trial registration: Dutch Trial Registration, NTR5932.
Conflict of interest statement
The PhD program of the corresponding author (T.L. Janssen) is funded by an ‘unrestricted grant’ by Amphia Fund for innovation. Limited financial support has been provided by Vifor Pharma Nederland B.V. All other authors declare that they have no competing interests. This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
References
-
- World Population Aging. New York: Department of Economic and Social Affairs: Population Division; 2015. Available from: http://www.un.org/en/development/desa/population/publications/pdf/ageing....
-
- IKNL. Nederlandse Kankerregistratie. Cijfers over kanker 2011–2018. [February 2018. ]. Available from: https://www.cijfersoverkanker.nl.
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
