

Technical Assessment of an Automated Treatment Planning on Dose Escalation of Pancreas Stereotactic Body Radiotherapy
- PMID: 31195891
- PMCID: PMC6572905
- DOI: 10.1177/1533033819851520
Technical Assessment of an Automated Treatment Planning on Dose Escalation of Pancreas Stereotactic Body Radiotherapy
Abstract
Background: Stereotactic body radiotherapy has been suggested to provide high rates of local control for locally advanced pancreatic cancer. However, the close proximity of highly radiosensitive normal tissues usually causes the labor-intensive planning process and may impede further escalation of the prescription dose.
Purpose: The present study aims to evaluate the consistency and efficiency of Pinnacle Auto-Planning for pancreas stereotactic body radiotherapy with original prescription and escalated prescription.
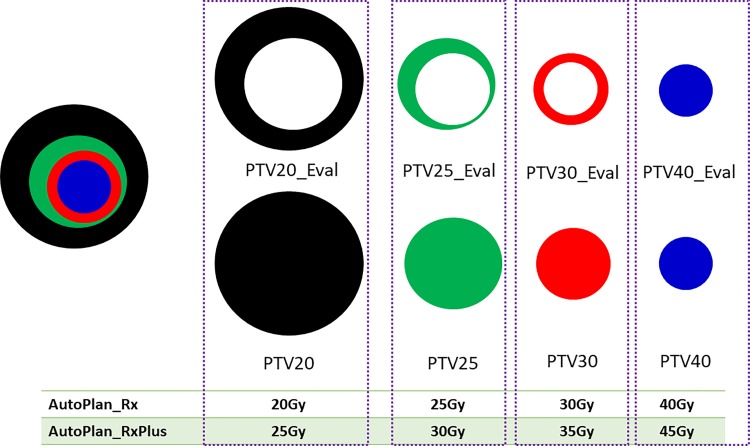
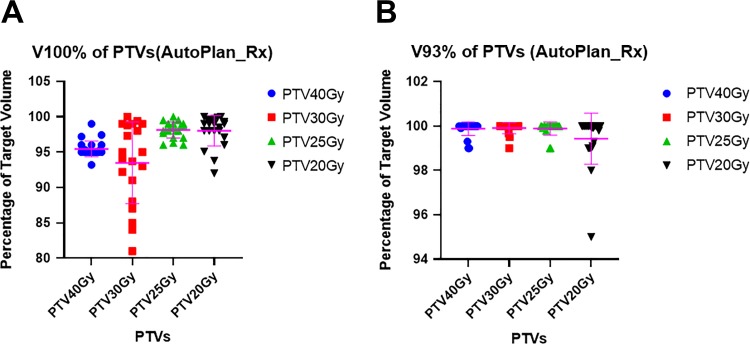
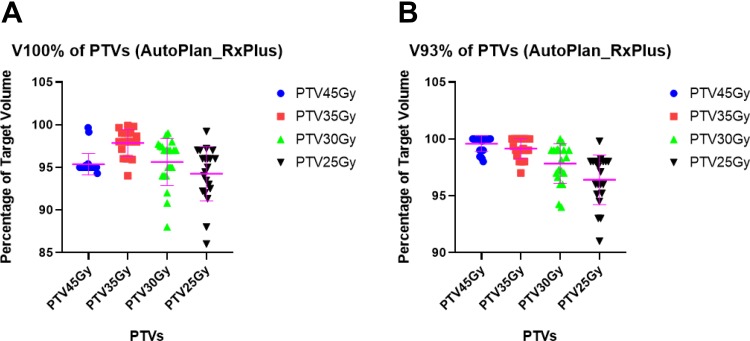
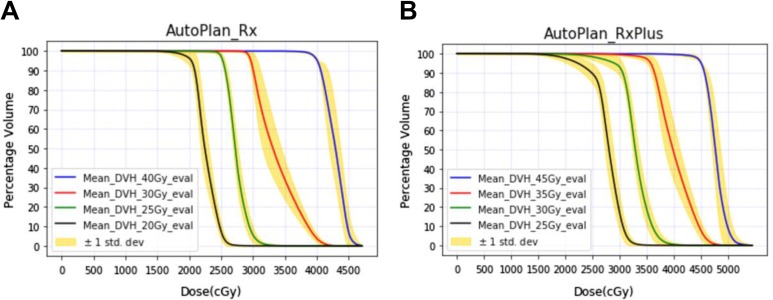
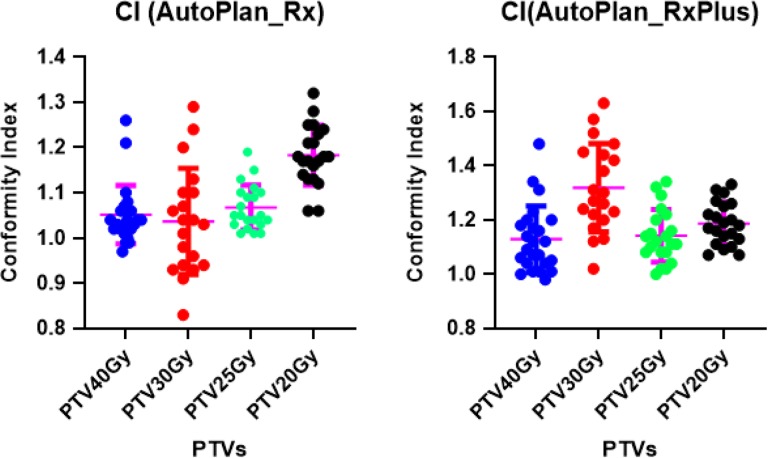
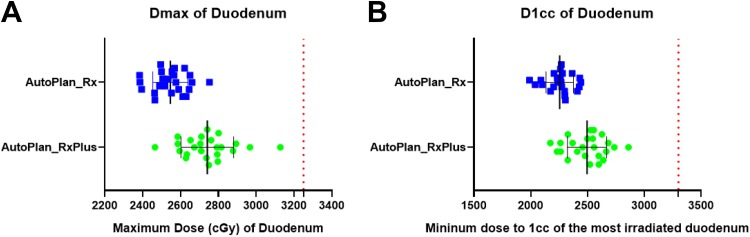
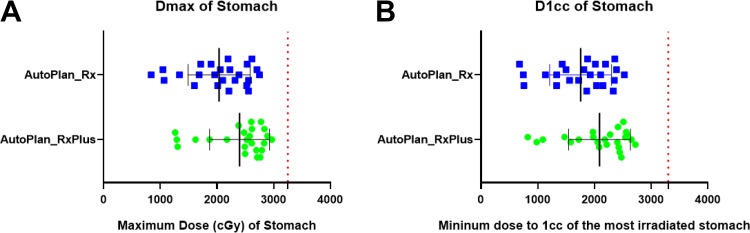
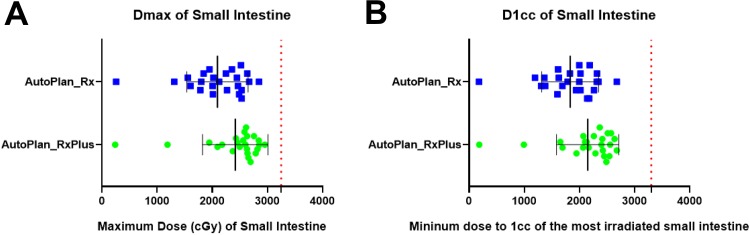
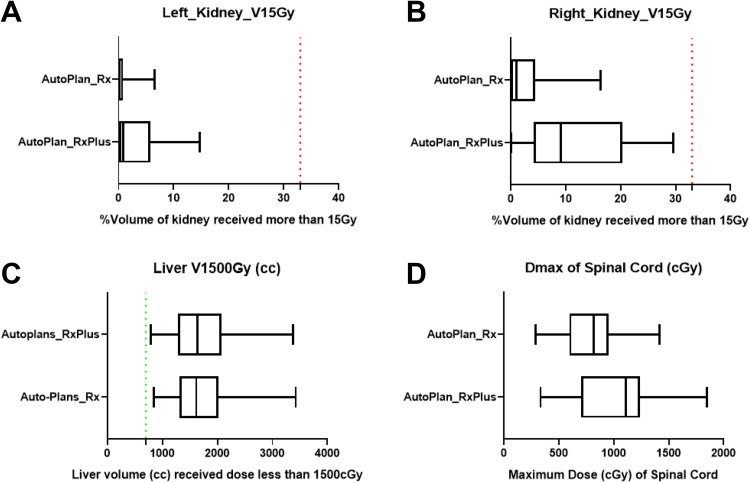
Methods: Twenty-four patients with pancreatic cancer treated with stereotactic body radiotherapy were studied retrospectively. The prescription is 40 Gy over 5 consecutive fractions. Most of patients (n = 21) also had 3 other different dose-level targets (6 Gy/fraction, 5 Gy/fraction, and 4 Gy/fraction). Two types of plans were generated by Pinnacle Auto-Planning with the original prescription (8 Gy/fraction, 6 Gy/fraction, 5 Gy/fraction, and 4 Gy/fraction) and escalated prescription (9 Gy/fraction, 7 Gy/fraction, 6 Gy/fraction, and 5 Gy/fraction), respectively. The same Auto-Planning template, including beam geometry, intensity-modulated radiotherapy objectives and intensity-modulated radiotherapy optimization parameters, were utilized for all the auto-plans in each prescription group. The intensity-modulated radiotherapy objectives do not include any manually created structures. Dosimetric parameters including percentage volume of PTV receiving 100% of the prescription dose, percentage volume of PTV receiving 93% of the prescription dose, and consistency of the dose-volume histograms of the target volumes were assessed. Dmax and D1 cc of highly radiosensitive organs were also evaluated.
Results: For all the pancreas stereotactic body radiotherapy plans with the original or escalated prescriptions, auto-plans met institutional dose constraints for critical organs, such as the duodenum, small intestine, and stomach. Furthermore, auto-plans resulted in acceptable planning target volume coverage for all targets with different prescription levels. All the plans were generated in a one-attempt manner, and very little human intervention is necessary to achieve such plan quality.
Conclusions: Pinnacle3 Auto-Planning consistently and efficiently generate acceptable treatment plans for multitarget pancreas stereotactic body radiotherapy with or without dose escalation and may play a more important role in treatment planning in the future.
Keywords: automated treatment planning; dose escalation; pancreatic cancer; personalized treatment; stereotactic body radiotherapy.
Conflict of interest statement
Figures
Similar articles
-
Assessment of Monte Carlo algorithm for compliance with RTOG 0915 dosimetric criteria in peripheral lung cancer patients treated with stereotactic body radiotherapy.J Appl Clin Med Phys. 2016 May 8;17(3):277-293. doi: 10.1120/jacmp.v17i3.6077. J Appl Clin Med Phys. 2016. PMID: 27167284 Free PMC article.
-
Dosimetric comparison of two treatment planning systems for spine SBRT.Med Dosim. 2020 Spring;45(1):77-84. doi: 10.1016/j.meddos.2019.07.001. Epub 2019 Aug 1. Med Dosim. 2020. PMID: 31376988
-
Interfractional dose variations in the stomach and the bowels during breathhold intensity-modulated radiotherapy for pancreatic cancer: Implications for a dose-escalation strategy.Med Phys. 2013 Feb;40(2):021701. doi: 10.1118/1.4773033. Med Phys. 2013. PMID: 23387724
-
NRG Oncology International Consensus Contouring Atlas on Target Volumes and Dosing Strategies for Dose-Escalated Pancreatic Cancer Radiation Therapy.Int J Radiat Oncol Biol Phys. 2025 Mar 15;121(4):918-929. doi: 10.1016/j.ijrobp.2024.10.026. Epub 2024 Nov 6. Int J Radiat Oncol Biol Phys. 2025. PMID: 39510320 Review.
-
Doses, fractionations, constraints for stereotactic radiotherapy.Rep Pract Oncol Radiother. 2022 Mar 22;27(1):10-14. doi: 10.5603/RPOR.a2021.0139. eCollection 2022. Rep Pract Oncol Radiother. 2022. PMID: 35402033 Free PMC article. Review.
Cited by
-
Radiotherapy Treatment Planning in the Age of AI: Are We Ready Yet?Technol Cancer Res Treat. 2019 Jan-Dec;18:1533033819894577. doi: 10.1177/1533033819894577. Technol Cancer Res Treat. 2019. PMID: 31858890 Free PMC article. No abstract available.
-
Automated treatment planning as a dose escalation strategy for stereotactic radiation therapy in pancreatic cancer.J Appl Clin Med Phys. 2020 Nov;21(11):48-57. doi: 10.1002/acm2.13025. Epub 2020 Oct 16. J Appl Clin Med Phys. 2020. PMID: 33063456 Free PMC article. Clinical Trial.
-
Evaluation of short-term gastrointestinal motion and its impact on dosimetric parameters in stereotactic body radiation therapy for pancreatic cancer.Clin Transl Radiat Oncol. 2023 Jan 7;39:100576. doi: 10.1016/j.ctro.2023.100576. eCollection 2023 Mar. Clin Transl Radiat Oncol. 2023. PMID: 36686564 Free PMC article.
-
Artificial Intelligence in Radiation Therapy.IEEE Trans Radiat Plasma Med Sci. 2022 Feb;6(2):158-181. doi: 10.1109/TRPMS.2021.3107454. Epub 2021 Aug 24. IEEE Trans Radiat Plasma Med Sci. 2022. PMID: 35992632 Free PMC article.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68(1):7–30. doi:10.3322/caac.21442 PubMed PMID: 29313949. - PubMed
-
- Trakul N, Koong AC, Chang DT. Stereotactic body radiotherapy in the treatment of pancreatic cancer. Semin Radiat Oncol. 2014;24(2):140–147. doi:10.1016/j.semradonc.2013.11.008 PubMed PMID: 24635871. - PubMed
-
- Saif MW. Pancreatic neoplasm in 2011: an update. JOP. 2011;12(4):316–321. PubMed PMID: 21737886. - PubMed
-
- Abrams RA, Lowy AM, O’Reilly EM, Wolff RA, Picozzi VJ, Pisters PW. Combined modality treatment of resectable and borderline resectable pancreas cancer: expert consensus statement. Ann Surg Oncol. 2009;16(7):1751–1756. doi:10.1245/s10434-009-0413-9 PubMed PMID: 19390900. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
