

Risk Factor for Residue After Uterine Artery Chemotherapy and Embolization in Combination with Dilatation and Curettage for Treating Caesarean Scar Pregnancy
- PMID: 31195943
- PMCID: PMC7040523
- DOI: 10.2174/1566524019666190612135728
Risk Factor for Residue After Uterine Artery Chemotherapy and Embolization in Combination with Dilatation and Curettage for Treating Caesarean Scar Pregnancy
Abstract
Objective: We aimed to investigate the potential risk factors for residual lesions after uterine artery chemotherapy and embolization (UACE) in combination with dilatation and curettage (D&C) in patients with cesarean scar pregnancy (CSP).
Settings: Retrospective case-control study.
Method: Univariate analysis and logistic analysis were applied to analyze these data to assess the risk factor of residue after UACE in combination with D&C.
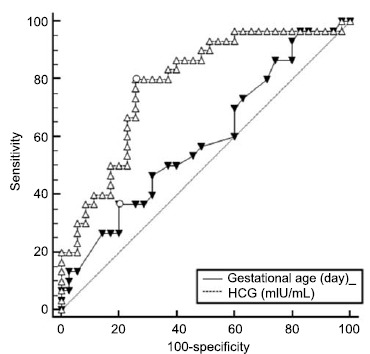
Results: Gestational age, human chorionic gonadotropin (HCG) level, and the gestation sac (GS) evagination to the bladder were the risk factors for the postoperative lesion. The most relevant was GS evagination to the bladder, followed by the preoperative HCG level and the gestational age. We defined the cut-off value of gestational age as 28 days with a sensitivity and specificity of 100 and 0, respectively.
Conclusion: In cases with GS evagination to bladder and HCG of >28,113.65 mIU/ml as well as a gestational age of >28 days, the possibility of residual lesions was high.
Keywords: Caesarean scar pregnancy; dilatation and curettage; residue; risk factors; uterine artery embolization..
Copyright© Bentham Science Publishers; For any queries, please email at epub@benthamscience.net.
Figures
Similar articles
-
hCG values and gestational sac size as indicators of successful systemic methotrexate treatment in cesarean scar pregnancy.Taiwan J Obstet Gynecol. 2021 May;60(3):454-457. doi: 10.1016/j.tjog.2021.03.011. Taiwan J Obstet Gynecol. 2021. PMID: 33966727
-
Role of collateral embolization in addition to uterine artery embolization followed by hysteroscopic curettage for the management of cesarean scar pregnancy.BMC Pregnancy Childbirth. 2019 Dec 16;19(1):502. doi: 10.1186/s12884-019-2590-2. BMC Pregnancy Childbirth. 2019. PMID: 31842804 Free PMC article.
-
[Feasibility of treatment of cesarean scar pregnancy with dilatation and curettage under ultrasound guidance].Zhonghua Yi Xue Za Zhi. 2015 Oct 6;95(37):3045-9. Zhonghua Yi Xue Za Zhi. 2015. PMID: 26814088 Chinese.
-
Clinical efficacy and safety between high-intensity focused ultrasound and uterine artery embolization for cesarean scar pregnancy: a systematic review and a meta-analysis.Ann Palliat Med. 2021 Jun;10(6):6379-6387. doi: 10.21037/apm-21-839. Ann Palliat Med. 2021. PMID: 34237960
-
Development of pseudoaneurysm in cesarean section scar pregnancy: a case report and literature review.J Med Ultrason (2001). 2018 Apr;45(2):357-362. doi: 10.1007/s10396-017-0836-z. Epub 2017 Nov 16. J Med Ultrason (2001). 2018. PMID: 29147816 Review.
Cited by
-
Advances in Treating Cesarean Scar Pregnancy: A Comprehensive Review of Techniques, Clinical Outcomes, and Fertility Preservation.Med Sci Monit. 2024 Apr 3;30:e943550. doi: 10.12659/MSM.943550. Med Sci Monit. 2024. PMID: 38566372 Free PMC article.
-
Clinical efficacy and safety of high-intensity focused ultrasound (HIFU) ablation in treatment of cesarean scar pregnancy (CSP) I and II.BMC Pregnancy Childbirth. 2022 Jul 30;22(1):607. doi: 10.1186/s12884-022-04848-z. BMC Pregnancy Childbirth. 2022. PMID: 35907811 Free PMC article.
References
-
- Timor-Tritsch I.E., Monteagudo A. Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta and cesarean scar pregnancy. A review. Am. J. Obstet. Gynecol. 2012;207:14–29. - PubMed
-
- Ko J.K., Li R.H., Cheung V.Y. Caesarean scar pregnancy: a 10-year experience. Aust. N. Z. J. Obstet. Gynaecol. 2015;55:64–69. - PubMed
-
- Sekiguchi A., Okuda N., Kawabata I., Nakai A., Takeshita T. Ultrasound detection of lacunae-like image of a cesarean scar pregnancy in the first trimester. J. Nippon Med. Sch. 2013;80:70–73. - PubMed
-
- Zhuang Y., Huang L. Uterine artery embolization compared with methotrexate for the management of pregnancy implanted within a cesarean scar. Am. J. Obstet. Gynecol. 2009;201:152.e151–152.e153. - PubMed
-
- Seow K.M., Wang P.H., Huang L.W., Hwang J.L. Transvaginal sono-guided aspiration of gestational sac concurrent with a local methotrexate injection for the treatment of unruptured cesarean scar pregnancy. Arch. Gynecol. Obstet. 2013;288:361–366. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical