

Hepatectomy for metachronous colorectal liver metastases following complete cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal metastases: a report of three cases
- PMID: 31196097
- PMCID: PMC6567639
- DOI: 10.1186/s12957-019-1646-0
Hepatectomy for metachronous colorectal liver metastases following complete cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal metastases: a report of three cases
Abstract
Background: Cytoreductive surgery (CRS) with hyperthermic intraperitoneal chemotherapy (HIPEC) for peritoneal metastasis (PM) from colorectal cancer (CRC) has been reported to substantially improve the prognosis and the quality of life of patients in comparison to systemic chemotherapy or palliative approaches. This study aimed to demonstrate the safety and feasibility of hepatectomy for metachronous liver metastases from CRC following CRS and HIPEC for PM on the basis of three case reports.
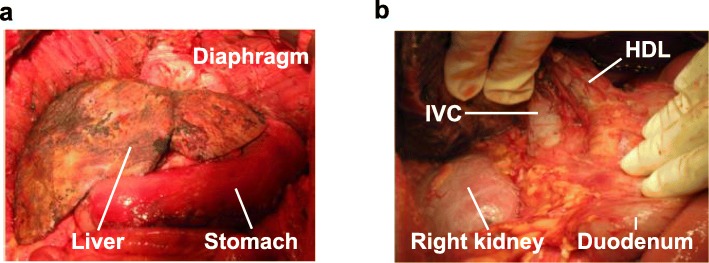
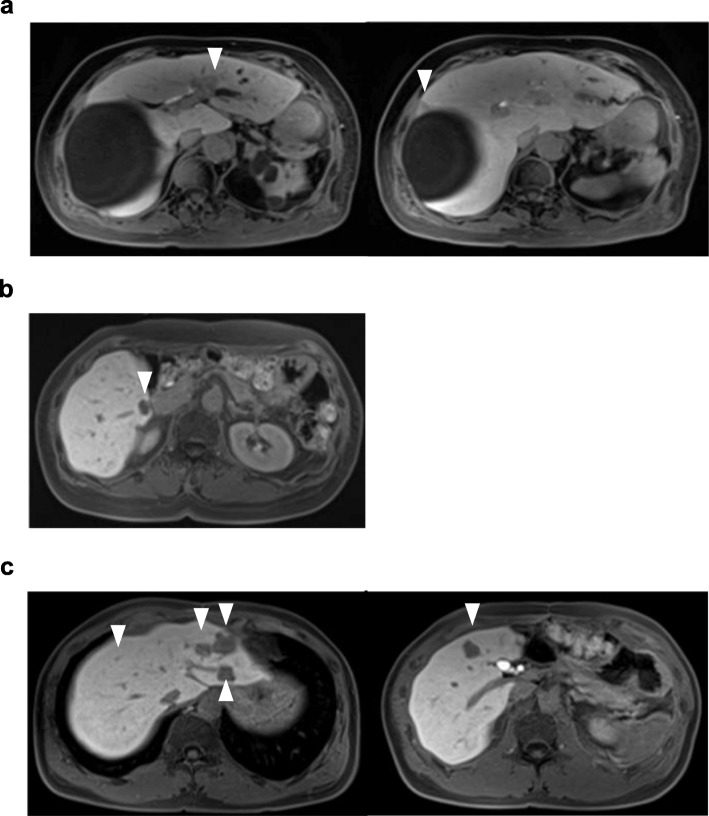
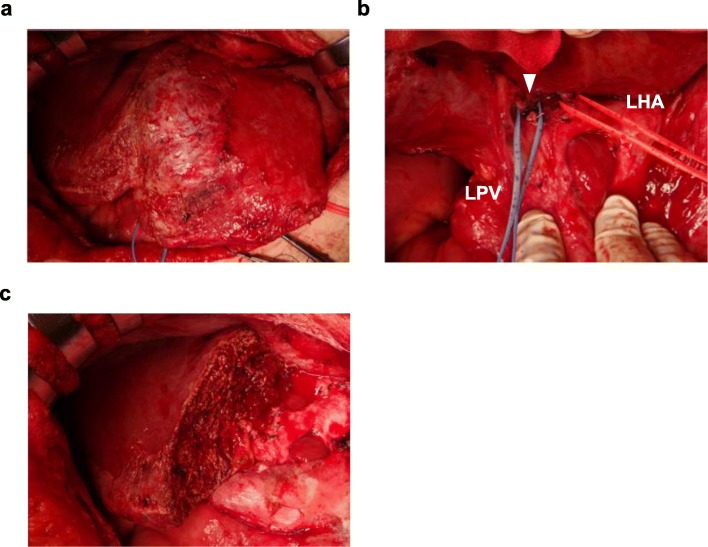
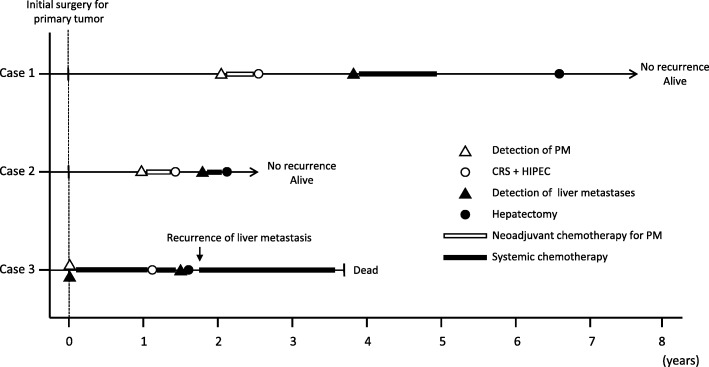
Case presentation: We describe three cases involving patients who underwent hepatectomy for metachronous liver metastases from CRC after CRS and HIPEC for PM. All patients underwent CRS and HIPEC after primary tumor resection, and hepatectomy was performed for the metachronous liver metastases after CRS and HIPEC. The hepatectomy procedures for cases 1, 2, and 3 were left hemihepatectomy and partial resection of S5, posterior sectionectomy, and left-lateral sectionectomy and partial resection of S5 and S8, respectively. Although adhesion of surrounding organs to the liver surface was observed on a broad level, dissections and hepatectomy could be performed safely. No recurrence was detected in cases 1 and 2 after hepatectomy. In case 3, liver metastases were detected from the time of the initial diagnosis of the primary tumor, and complete remission was achieved once with systemic chemotherapy. Although we performed hepatectomy for the recurrence of liver metastases after complete remission, early re-recurrence was observed after hepatectomy.
Conclusions: Hepatectomy for metachronous liver metastases after CRS and HIPEC for PM could be a multi-modality treatment option for CRC recurrence.
Keywords: Colorectal cancer; Cytoreductive surgery; Hepatectomy; Hyperthermic intraperitoneal chemotherapy; Liver metastases; Multi-modality treatment; Peritoneal metastases.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
"En bloc" caudate lobe and inferior vena cava resection following cytoreductive surgery and hyperthermic intraperitoneal chemotherapy for peritoneal and liver metastasis of colorectal cancer.World J Gastroenterol. 2016 Dec 14;22(46):10249-10253. doi: 10.3748/wjg.v22.i46.10249. World J Gastroenterol. 2016. PMID: 28028374 Free PMC article.
-
Impact of Synchronous Versus Metachronous Onset of Colorectal Peritoneal Metastases on Survival Outcomes After Cytoreductive Surgery (CRS) with Hyperthermic Intraperitoneal Chemotherapy (HIPEC): A Multicenter, Retrospective, Observational Study.Ann Surg Oncol. 2019 Jul;26(7):2210-2221. doi: 10.1245/s10434-019-07294-y. Epub 2019 Mar 15. Ann Surg Oncol. 2019. PMID: 30877495 Free PMC article.
-
Treatment of intraoperatively detected peritoneal carcinomatosis of colorectal origin with cytoreductive surgery and intraperitoneal chemotherapy.World J Surg Oncol. 2018 Mar 27;16(1):70. doi: 10.1186/s12957-018-1369-7. World J Surg Oncol. 2018. PMID: 29587771 Free PMC article.
-
Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (HIPEC) for colorectal and appendiceal peritoneal metastases - The Hong Kong experience and literature review.Asian J Surg. 2021 Jan;44(1):221-228. doi: 10.1016/j.asjsur.2020.05.010. Epub 2020 Jun 27. Asian J Surg. 2021. PMID: 32605790 Review.
-
Indications for hyperthermic intraperitoneal chemotherapy with cytoreductive surgery: a systematic review.Eur J Cancer. 2020 Mar;127:76-95. doi: 10.1016/j.ejca.2019.10.034. Epub 2020 Jan 24. Eur J Cancer. 2020. PMID: 31986452
Cited by
-
Expanding the horizons of cytoreductive surgery-hyperthermic intraperitoneal chemotherapy and liver resection for colorectal peritoneal and liver metastases.Hepatobiliary Surg Nutr. 2025 Jun 1;14(3):473-475. doi: 10.21037/hbsn-2025-189. Epub 2025 May 21. Hepatobiliary Surg Nutr. 2025. PMID: 40529911 Free PMC article. No abstract available.
-
Clinical outcomes of complete cytoreduction with concurrent liver resection followed by hyperthermic intraperitoneal chemotherapy for synchronous peritoneal and liver metastatic colorectal cancer.World J Surg Oncol. 2019 Dec 11;17(1):214. doi: 10.1186/s12957-019-1746-x. World J Surg Oncol. 2019. PMID: 31829188 Free PMC article.
-
Perioperative and Oncological Outcomes of Combined Hepatectomy with Complete Cytoreduction and Hyperthermic Intraperitoneal Chemotherapy for Metastatic Colorectal Cancer.Ann Surg Oncol. 2021 Jun;28(6):3320-3329. doi: 10.1245/s10434-020-09165-3. Epub 2020 Sep 23. Ann Surg Oncol. 2021. PMID: 32968959
References
-
- Sadeghi B, Arvieux C, Glehen O, Beaujard AC, Rivoire M, Baulieux J, Fontaumard E, Brachet A, Caillot JL, Faure JL. Peritoneal carcinomatosis from non-gynecologic malignancies: results of the EVOCAPE 1 multicentric prospective study. Cancer. 2000;88:358–363. doi: 10.1002/(SICI)1097-0142(20000115)88:2<358::AID-CNCR16>3.0.CO;2-O. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
