

Management of orbital invasion in esthesioneuroblastoma: 14 years' experience
- PMID: 31196122
- PMCID: PMC6567903
- DOI: 10.1186/s13014-019-1313-1
Management of orbital invasion in esthesioneuroblastoma: 14 years' experience
Abstract
Background: There is a scarcity of data about the prognostic value of orbital invasion in esthesioneuroblastoma (ENB), as well as about its management strategies. Indications for the preservation of orbital contents remain controversial, and the evaluation of orbital invasion has been ill defined.
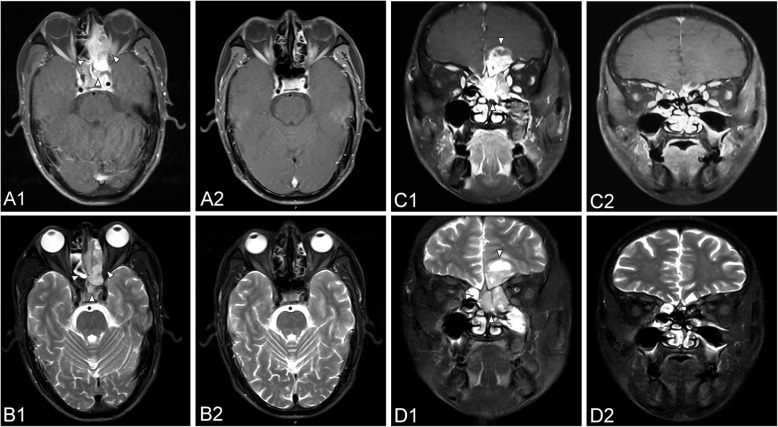
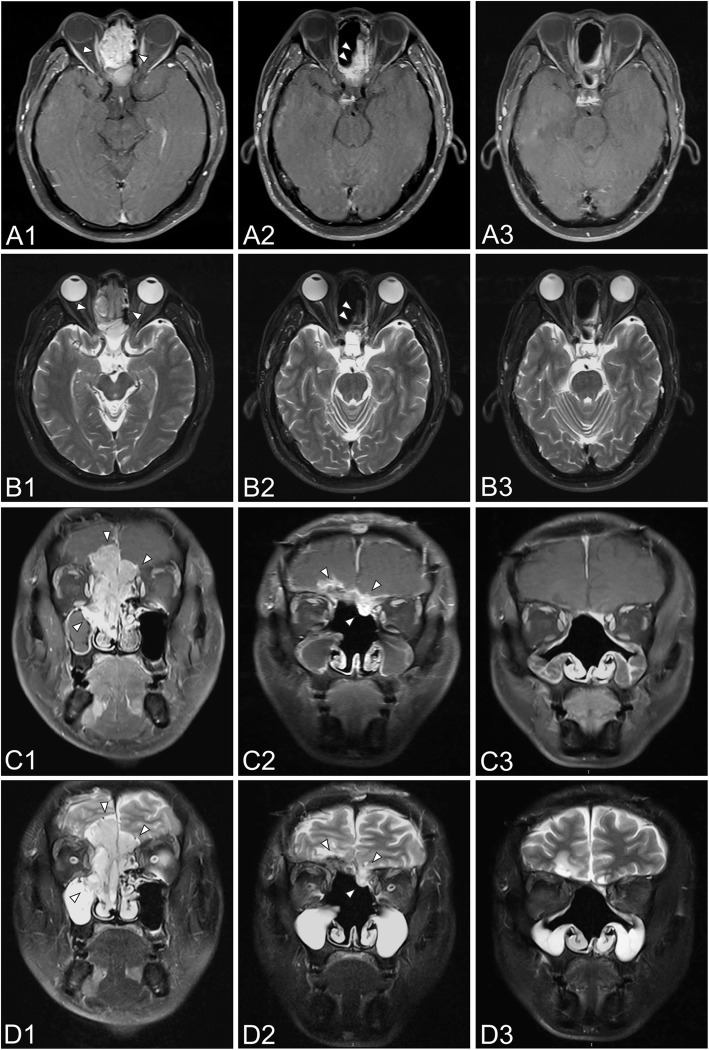
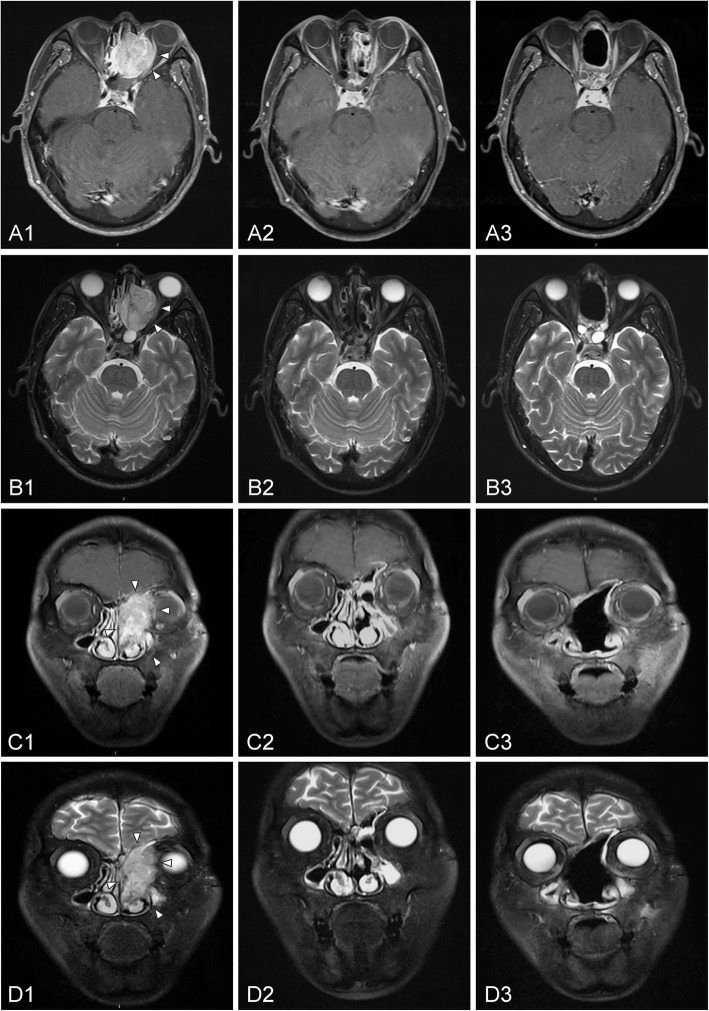
Methods: This retrospective analysis contained 60 ENB patients with orbital invasion who underwent radiotherapy with or without surgery over the past 14 years. Orbital invasion was classified into three grades.
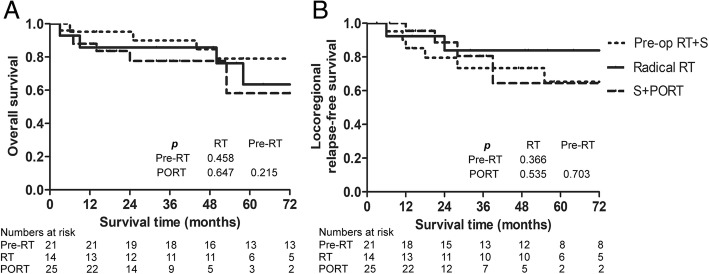
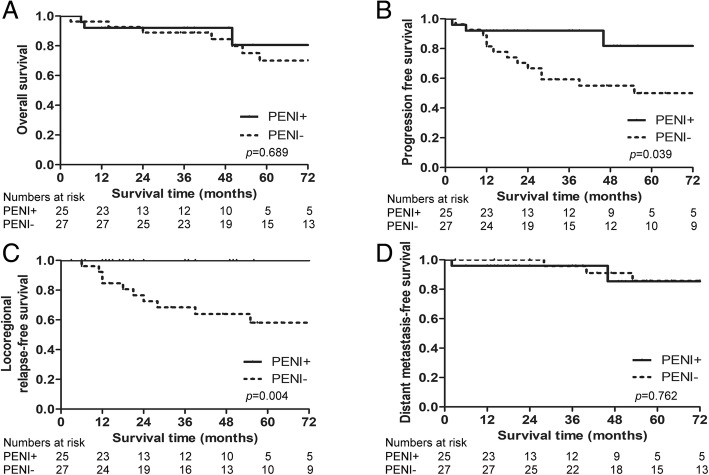
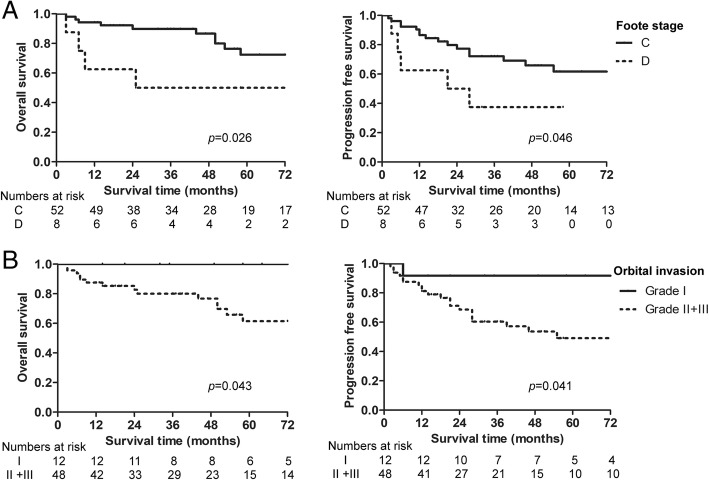
Results: There were 52 patients at stage C and 8 at stage D, according to Foote classifications. Grade I, grade II and grade III orbital invasion was detected in 12, 23, and 25 patients, respectively. The median follow-up was 57 months (IQR 32-95 months). Fourteen patients received radical radiotherapy, with a 5-year overall survival (OS) of 63.5%; 46 received surgery plus radiation, with a 5-year OS of 70.7%; and the difference was not statistically significant (p = 0.847). Orbital preservation was feasible in 100% of cases, including 18 cases that extended to extraocular muscles or the eye globe. Five-year locoregional relapse-free survival was 100% in patients with prophylactic elective neck irradiation (PENI) and 58.1% in patients without PENI (p = 0.004). Univariate analysis showed that grade II/III orbital invasion was associated with poorer OS and progression-free survival. Neck metastasis (with a Foote stage of D) was independently associated with shorter OS and distant metastasis-free survival in multivariate analysis.
Conclusions: Our data suggested that primary radiotherapy achieved comparable survival to surgery plus radiotherapy in advanced ENB. Invasion of either the extraocular muscles or the eye globe is not a contraindication for eye-sparing surgery. Orbital invasion in grade II/III was significantly associated with adverse survival outcomes. Prophylactic radiotherapy to the neck with N0 significantly reduces the risk of regional recurrence.
Keywords: Esthesioneuroblastoma; Orbital invasion; Orbital preservation; Prognostic factors; Radiotherapy.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Long-term analysis of multimodality treatment outcomes and prognosis of esthesioneuroblastomas: a single center results of 138 patients.Radiat Oncol. 2020 Sep 18;15(1):219. doi: 10.1186/s13014-020-01667-4. Radiat Oncol. 2020. PMID: 32948223 Free PMC article. Clinical Trial.
-
Management of orbital invasion in sinonasal squamous cell carcinoma: 15 years' experience.Int Forum Allergy Rhinol. 2020 Feb;10(2):243-255. doi: 10.1002/alr.22465. Epub 2019 Nov 22. Int Forum Allergy Rhinol. 2020. PMID: 31756058
-
Optimal treatment and prognostic factors for esthesioneuroblastoma: retrospective analysis of 187 Chinese patients.BMC Cancer. 2017 Apr 11;17(1):254. doi: 10.1186/s12885-017-3247-z. BMC Cancer. 2017. PMID: 28399835 Free PMC article.
-
Esthesioneuroblastoma: a meta-analysis and review.Lancet Oncol. 2001 Nov;2(11):683-90. doi: 10.1016/S1470-2045(01)00558-7. Lancet Oncol. 2001. PMID: 11902539 Review.
-
Consolidating the Hyams grading system in esthesioneuroblastoma - an individual participant data meta-analysis.J Neurooncol. 2021 May;153(1):15-22. doi: 10.1007/s11060-021-03746-2. Epub 2021 Mar 26. J Neurooncol. 2021. PMID: 33770323 Review.
Cited by
-
Development and validation of a postoperative nomogram for predicting overall survival after endoscopic surgical management of olfactory neuroblastoma.EClinicalMedicine. 2020 Nov 30;29-30:100577. doi: 10.1016/j.eclinm.2020.100577. eCollection 2020 Dec. EClinicalMedicine. 2020. PMID: 33305194 Free PMC article.
-
Management of Esthesioneuroblastoma: A Retrospective Study of 6 Cases and Literature Review.Case Rep Oncol. 2022 Mar 10;15(1):176-186. doi: 10.1159/000521736. eCollection 2022 Jan-Apr. Case Rep Oncol. 2022. PMID: 35431860 Free PMC article.
-
Comparative outcome of surgical and nonsurgical therapy for T4bN0M0 sinonasal squamous cell carcinomas.Eur Arch Otorhinolaryngol. 2019 Nov;276(11):3113-3122. doi: 10.1007/s00405-019-05601-7. Epub 2019 Aug 26. Eur Arch Otorhinolaryngol. 2019. PMID: 31451900
-
Long-Term Survival Outcomes and Treatment Experience of 64 Patients With Esthesioneuroblastoma.Front Oncol. 2021 Mar 4;11:624960. doi: 10.3389/fonc.2021.624960. eCollection 2021. Front Oncol. 2021. PMID: 33747939 Free PMC article.
-
Long-term analysis of multimodality treatment outcomes and prognosis of esthesioneuroblastomas: a single center results of 138 patients.Radiat Oncol. 2020 Sep 18;15(1):219. doi: 10.1186/s13014-020-01667-4. Radiat Oncol. 2020. PMID: 32948223 Free PMC article. Clinical Trial.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
