

Ion channels and transporters in diabetic kidney disease
- PMID: 31196609
- PMCID: PMC6815098
- DOI: 10.1016/bs.ctm.2019.01.001
Ion channels and transporters in diabetic kidney disease
Abstract
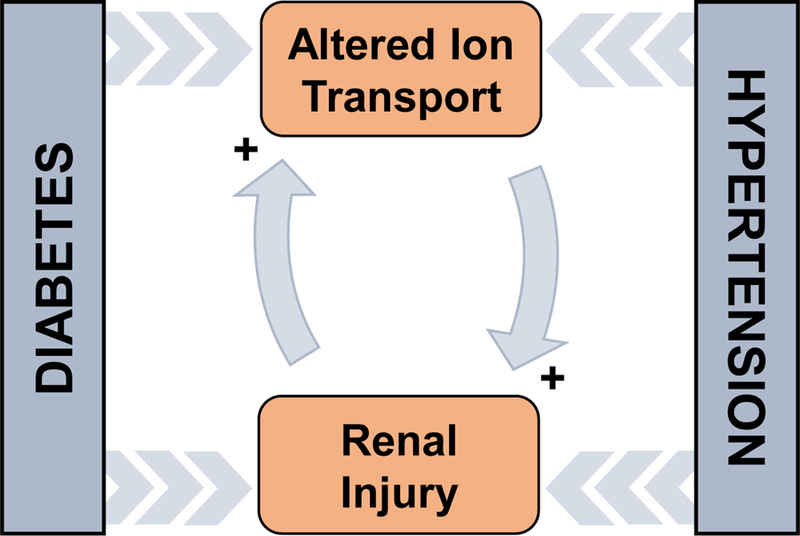
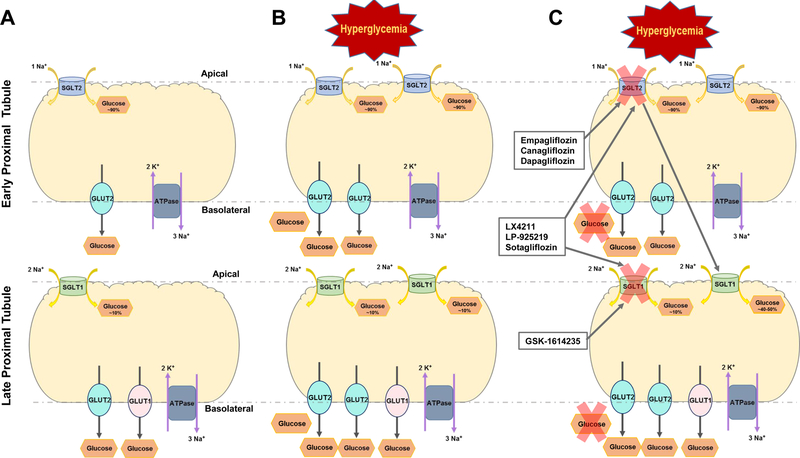
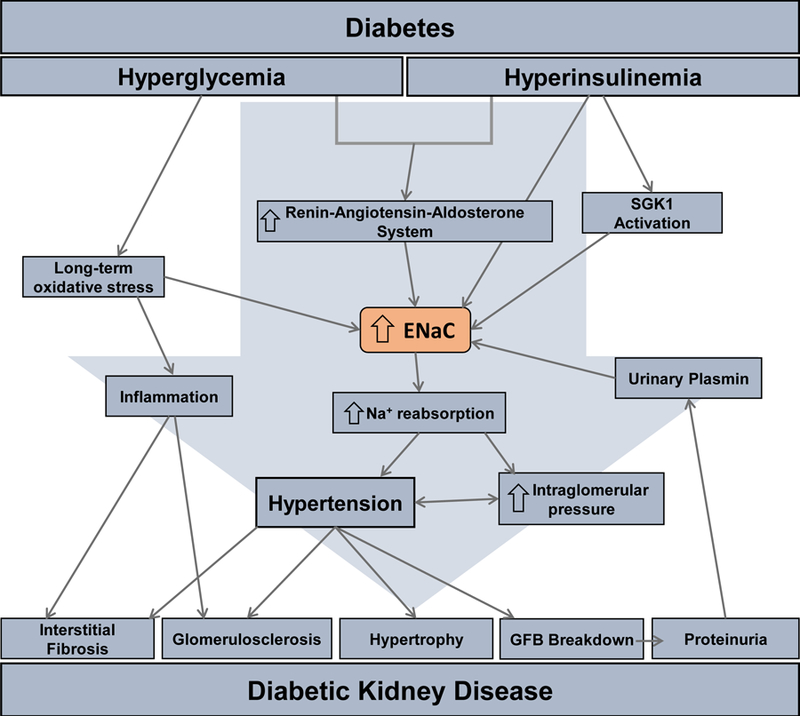
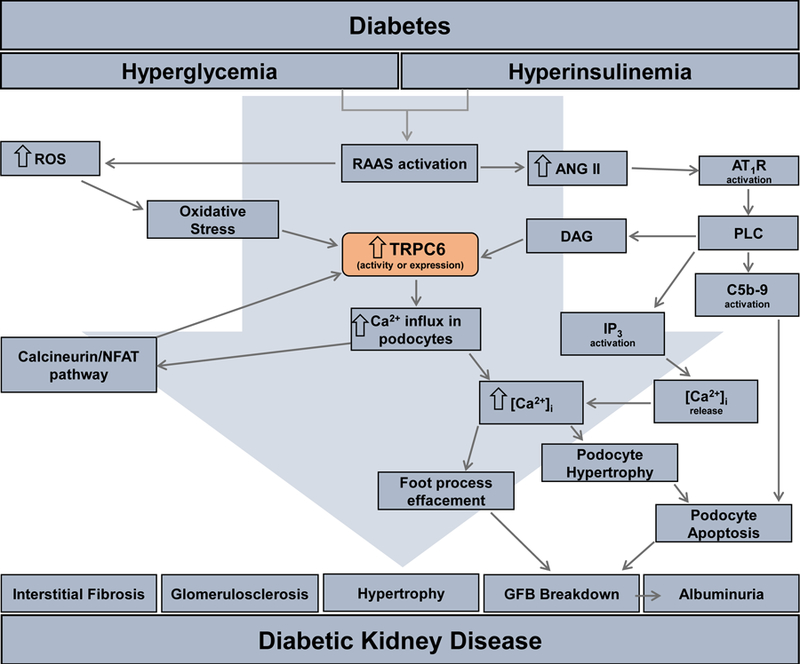
Type 1 and 2 diabetes mellitus are major medical epidemics affecting millions of patients worldwide. Diabetes mellitus is the leading cause of diabetic kidney disease (DKD), which is the most common cause of end-stage renal disease (ESRD). DKD is associated with significant changes in renal hemodynamics and electrolyte transport. Alterations in renal ion transport triggered by pathophysiological conditions in diabetes can exacerbate hypertension, accelerate renal injury, and are integral to the development of DKD. Renal ion transporters and electrolyte homeostasis play a fundamental role in functional changes and injury to the kidney during DKD. With the large number of ion transporters involved in DKD, understanding the roles of individual transporters as well as the complex cascades through which they interact is essential in the development of effective treatments for patients suffering from this disease. This chapter aims to gather current knowledge of the major renal ion transporters with altered expression and activity under diabetic conditions, and provide a comprehensive overview of their interactions and collective functions in DKD.
Keywords: Diabetic kidney disease; Diabetic nephropathy; ENaC; K(ATP) channel; NHE; SGLT2; TRPC6; TRPM6.
© 2019 Elsevier Inc. All rights reserved.
Figures

References
-
- Andersen H, Friis UG, Hansen PB, Svenningsen P, Henriksen JE, & Jensen BL (2015). Diabetic nephropathy is associated with increased urine excretion of proteases plasmin, prostasin and urokinase and activation of amiloride-sensitive current in collecting duct cells. Nephrol Dial Transplant, 30(5), 781–789. 10.1093/ndt/gfu402 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
