

Introduction of anti-TNF therapy has not yielded expected declines in hospitalisation and intestinal resection rates in inflammatory bowel diseases: a population-based interrupted time series study
- PMID: 31196874
- PMCID: PMC6984056
- DOI: 10.1136/gutjnl-2019-318440
Introduction of anti-TNF therapy has not yielded expected declines in hospitalisation and intestinal resection rates in inflammatory bowel diseases: a population-based interrupted time series study
Abstract
Objectives: To better understand the real-world impact of biologic therapy in persons with Crohn's disease (CD) and ulcerative colitis (UC), we evaluated the effect of marketplace introduction of infliximab on the population rates of hospitalisations and surgeries and public payer drug costs.
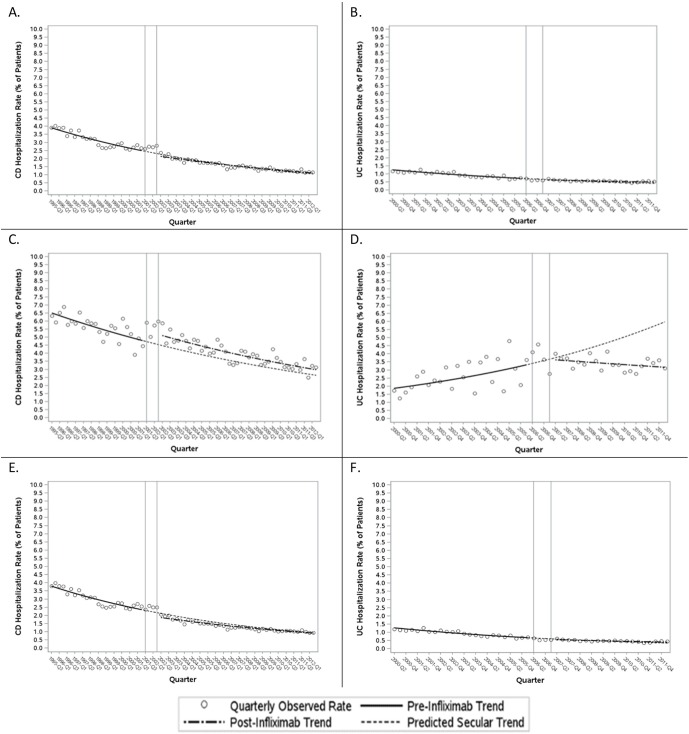
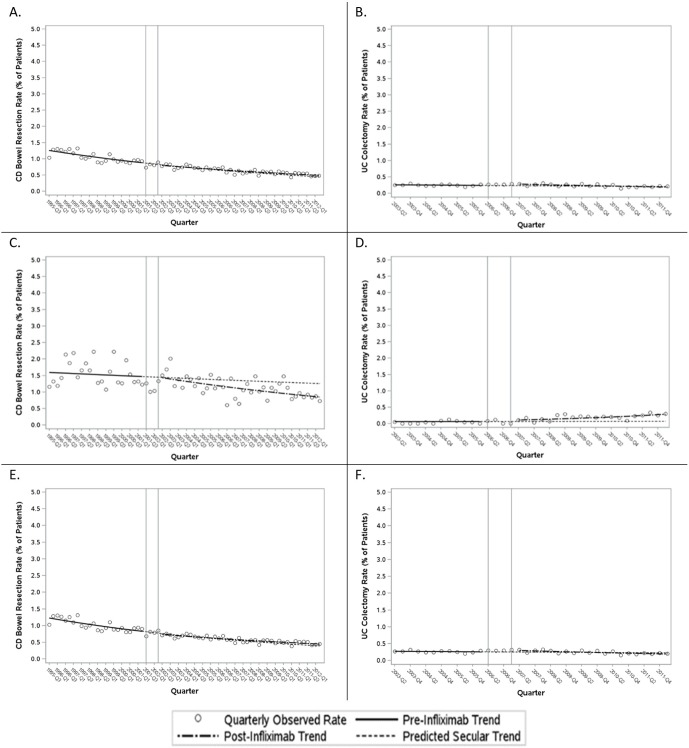
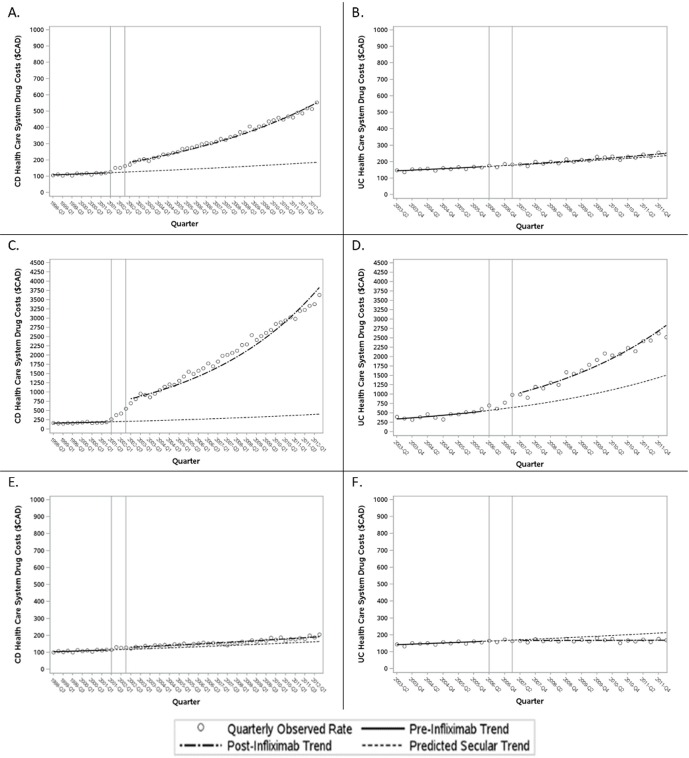
Design: We used health administrative data to study adult persons with CD and UC living in Ontario, Canada between 1995 and 2012. We used an interrupted time series design with segmented regression analysis to evaluate the impact of infliximab introduction on the rates of IBD-related hospitalisations, intestinal resections and public payer drug costs over 10 years among patients with CD and 5 years among patients with UC, allowing for a 1-year transition.
Results: Relative to what would have been expected in the absence of infliximab, marketplace introduction of infliximab did not produce significant declines in the rates of CD-related hospitalisations (OR at the last observation quarter 1.06, 95% CI 0.811 to 1.39) or intestinal resections (OR 1.10, 95% CI 0.810 to 1.50), or in the rates of UC-related hospitalisations (OR 1.22, 95% CI 1.07 to 1.39) or colectomies (OR 0.933, 95% CI 0.54 to 1.61). The findings were similar among infliximab users, except that hospitalisation rates declined substantially among UC patients following marketplace introduction of infliximab (OR 0.515, 95% CI 0.342 to 0.777). There was a threefold rise over expected trends in public payer drug cost among patients with CD following infliximab introduction (OR 2.98,95% CI 2.29 to 3.86), suggesting robust market penetration in this group, but no significant change among patients with UC (OR 1.06, 95% CI 0.955 to 1.18).
Conclusions: Marketplace introduction of infliximab has not yielded anticipated reductions in the population rates of IBD-related hospitalisations or intestinal resections, despite robust market penetration among patients with CD. Misguided use of infliximab in CD patients and underuse of infliximab in UC patients may largely explain our study findings.
Keywords: crohn’s disease; inflammatory bowel disease; surgery for Ibd; ulcerative colitis.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: COI Statement: SKM has received honoraria for speaking or consultancy from AbbVie, Janssen, Takeda, Pfizer, Shire and Ferring. JB has no conflicts of interest. EIB has no conflicts of interest. CNB has served on advisory boards of AbbVie Canada, Ferring Canada, Janssen Canada, Napo Pharmaceuticals, Pfizer Canada, Shire Canada, Takeda Canada, and has consulted to 4D Pharma and Mylan Pharmaceuticals. He has received unrestricted educational grants from AbbVie Canada, Janssen Canada, Shire Canada and Takeda Canada. He has been on speaker’s bureau of Ferring Canada and Shire Canada. GG has received honoraria for speaking or consultancy from AbbVie, Janssen, Pfizer and Takeda, and research support from Janssen, AbbVie, GlaxoSmithKline, Merck and Shire. He shares ownership of a patent: Treatment ofInflammatory Disorders, Autoimmune Disease and PBC . UTI Limited Partnership, assignee, Patent 62/555,397, 7 September 2017. JDMcC has received honoraria for speaking or consultancy from AbbVie, Janssen, Takeda, Pfizer, Shire and Ferring. HS has served on advisory boards of Ferring Canada, Takeda Canada, Merck Canada and received research funding from Merck Canada. LT has received research funding from Janssen Canada, and served on advisory boards for AbbVie Canada, Takeda Canada, Merck Canada, Pfizer Canada and Mallinckrodt USA.
Figures
Comment in
-
Intestinal resection rates in Crohn's disease decline across two different epidemiological areas: a consistent observation not merely due to introduction of anti-TNFα.Gut. 2020 Sep;69(9):1. doi: 10.1136/gutjnl-2019-319321. Epub 2019 Aug 14. Gut. 2020. PMID: 31413165 Free PMC article. No abstract available.
-
The cost and benefit of anti-TNF therapy from a population perspective-for what it's worth.Ann Transl Med. 2019 Dec;7(Suppl 8):S388. doi: 10.21037/atm.2019.12.86. Ann Transl Med. 2019. PMID: 32016106 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources