

Trends in kidney function testing in UK primary care since the introduction of the quality and outcomes framework: a retrospective cohort study using CPRD
- PMID: 31196901
- PMCID: PMC6575820
- DOI: 10.1136/bmjopen-2018-028062
Trends in kidney function testing in UK primary care since the introduction of the quality and outcomes framework: a retrospective cohort study using CPRD
Erratum in
-
Correction: Trends in kidney function testing in UK primary care since the introduction of the quality and outcomes framework: a retrospective cohort study using CPRD.BMJ Open. 2019 Jul 1;9(7):e028062corr1. doi: 10.1136/bmjopen-2018-028062corr1. BMJ Open. 2019. PMID: 31266844 Free PMC article. No abstract available.
Abstract
Objectives: To characterise serum creatinine and urinary protein testing in UK general practices from 2005 to 2013 and to examine how the frequency of testing varies across demographic factors, with the presence of chronic conditions and with the prescribing of drugs for which kidney function monitoring is recommended.
Design: Retrospective open cohort study.
Setting: Routinely collected data from 630 UK general practices contributing to the Clinical Practice Research Datalink.
Participants: 4 573 275 patients aged over 18 years registered at up-to-standard practices between 1 April 2005 and 31 March 2013. At study entry, no patients were kidney transplant donors or recipients, pregnant or on dialysis.
Primary outcome measures: The rate of serum creatinine and urinary protein testing per year and the percentage of patients with isolated and repeated testing per year.
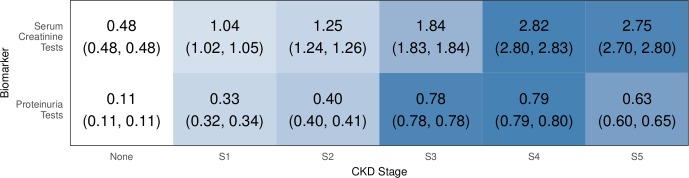
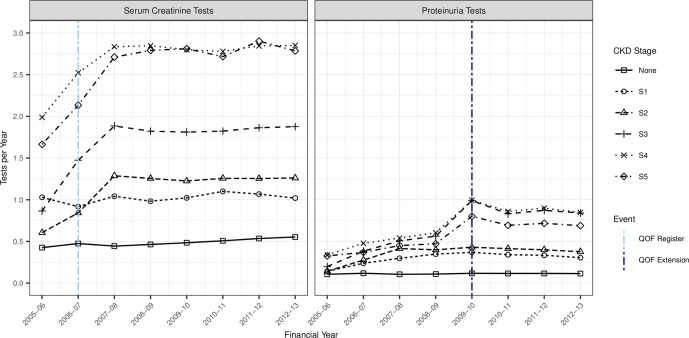
Results: The rate of serum creatinine testing increased linearly across all age groups. The rate of proteinuria testing increased sharply in the 2009-2010 financial year but only for patients aged 60 years or over. For patients with established chronic kidney disease (CKD), creatinine testing increased rapidly in 2006-2007 and 2007-2008, and proteinuria testing in 2009-2010, reflecting the introduction of Quality and Outcomes Framework indicators. In adjusted analyses, CKD Read codes were associated with up to a twofold increase in the rate of serum creatinine testing, while other chronic conditions and potentially nephrotoxic drugs were associated with up to a sixfold increase. Regional variation in serum creatinine testing reflected country boundaries.
Conclusions: Over a nine-year period, there have been increases in the numbers of patients having kidney function tests annually and in the frequency of testing. Changes in the recommended management of CKD in primary care were the primary determinant, and increases persist even after controlling for demographic and patient-level factors. Future studies should address whether increased testing has led to better outcomes.
Keywords: chronic kidney disease; kidney function; monitoring; primary care; proteinuria; serum creatinine.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: NRH is currently employed by Bristol-Meyers Squibb Limited, a company that manufactures ACE inhibitors, which are drugs indicated in the treatment of chronic kidney disease, when present in conjunction with other comorbidities such as type 2 diabetes. CT reports speaker fees from Vifor and Novartis and non-financial support from Roche outside of the submitted work. All other authors declare no conflicts of interest.
Figures





References
-
- National Institute for Health and Care Excellence, “Chronic kidney disease in adults: assessment and management. Clinical guideline [CG182]. 2014. https://www.nice.org.uk/guidance/cg182. - PubMed
-
- National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 2002;39(2 Suppl 1):S1–S266. - PubMed
-
- Department of Health, The National Services Framework for Renal Services. Part One: Dialysis and Transplantation, 2004.
-
- British Medical Association. “Revisions to the GMS contract 2006/07. 2006. http://www.nhsemployers.org/-/media/Employers/Documents/Primary-care-con....
-
- National Institute for Health and Care Excellence. NICE Clinical Guideline 73: Chronic Kidney Disease: Early Identification and Management of Chronic Kidney Disease in Adults in Primary and Secondary Care. 2008. https://www.nice.org.uk/guidance/CG73.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous