

Effects of Treatment of Metabolic Acidosis in CKD: A Systematic Review and Meta-Analysis
- PMID: 31196951
- PMCID: PMC6625635
- DOI: 10.2215/CJN.13091118
Effects of Treatment of Metabolic Acidosis in CKD: A Systematic Review and Meta-Analysis
Abstract
Background and objectives: Metabolic acidosis is associated with progression of CKD and has significant adverse effects on muscle and bone. A systematic review and meta-analysis was conducted to evaluate the benefits and risks of metabolic acidosis treatment with oral alkali supplementation or a reduction of dietary acid intake in those with CKD.
Design, setting, participants, & measurements: MEDLINE, Embase, and Cochrane CENTRAL were searched for relevant trials in patients with stage 3-5 CKD and metabolic acidosis (<22 mEq/L) or low-normal serum bicarbonate (22-24 mEq/L). Data were pooled in a meta-analysis with results expressed as weighted mean difference for continuous outcomes and relative risk for categorical outcomes with 95% confidence intervals (95% CIs), using a random effects model. Study quality and strength of evidence were assessed using Cochrane risk of bias and the Grading of Recommendations Assessment, Development and Evaluation criteria.
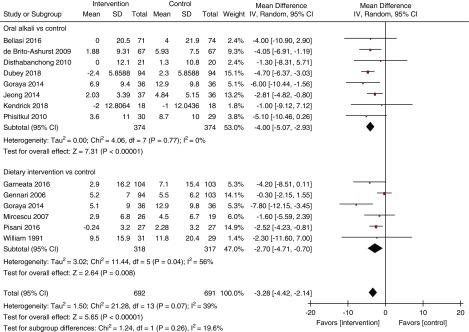
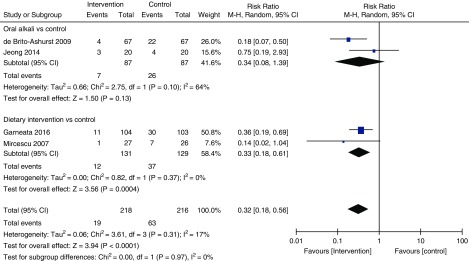
Results: Fourteen clinical trials were included (n=1394 participants). Treatment of metabolic acidosis with oral alkali supplementation or a reduction of dietary acid intake increased serum bicarbonate levels (14 studies, 1378 patients, mean difference 3.33 mEq/L, 95% CI, 2.37 to 4.29) and resulted in a slower decline in eGFR (13 studies, 1329 patients, mean difference -3.28 ml/min per 1.73 m2, 95% CI, -4.42 to -2.14; moderate certainty) and a reduction in urinary albumin excretion (very-low certainty), along with a reduction in the risk of progression to ESKD (relative risk, 0.32; 95% CI, 0.18 to 0.56; low certainty). Oral alkali supplementation was associated with worsening hypertension or the requirement for increased antihypertensive therapy (very-low certainty).
Conclusions: Low-to-moderate certainty evidence suggest that oral alkali supplementation or a reduction in dietary acid intake may slow the rate of kidney function decline and potentially reduce the risk of ESKD in patients with CKD and metabolic acidosis.
Keywords: Albumins; Alkalies; Antihypertensive Agents; Bias; Bicarbonates; Confidence Intervals; Kidney Failure, Chronic; Renal Insufficiency, Chronic; Risk Assessment; acidosis; chronic metabolic acidosis; glomerular filtration rate; hypertension; kidney disease; sodium bicarbonate.
Copyright © 2019 by the American Society of Nephrology.
Figures



Similar articles
-
Low Serum Bicarbonate and CKD Progression in Children.Clin J Am Soc Nephrol. 2020 Jun 8;15(6):755-765. doi: 10.2215/CJN.07060619. Epub 2020 May 28. Clin J Am Soc Nephrol. 2020. PMID: 32467307 Free PMC article.
-
Effects of oral alkali drug therapy on clinical outcomes in pre-dialysis chronic kidney disease patients: a systematic review and meta-analysis.Ren Fail. 2022 Dec;44(1):106-115. doi: 10.1080/0886022X.2021.2023023. Ren Fail. 2022. PMID: 35176947 Free PMC article.
-
Impact of Serum Bicarbonate Levels on Muscle Mass and Kidney Function in Pre-Dialysis Chronic Kidney Disease Patients.Am J Nephrol. 2020;51(1):24-34. doi: 10.1159/000504557. Epub 2019 Nov 21. Am J Nephrol. 2020. PMID: 31752000 Clinical Trial.
-
Metabolic acidosis is associated with increased risk of adverse kidney outcomes and mortality in patients with non-dialysis dependent chronic kidney disease: an observational cohort study.BMC Nephrol. 2021 May 19;22(1):185. doi: 10.1186/s12882-021-02385-z. BMC Nephrol. 2021. PMID: 34011303 Free PMC article.
-
Immunosuppressive agents for treating IgA nephropathy.Cochrane Database Syst Rev. 2020 Mar 12;3(3):CD003965. doi: 10.1002/14651858.CD003965.pub3. Cochrane Database Syst Rev. 2020. PMID: 32162319 Free PMC article.
Cited by
-
Dietary acid load in health and disease.Pflugers Arch. 2024 Apr;476(4):427-443. doi: 10.1007/s00424-024-02910-7. Epub 2024 Jan 29. Pflugers Arch. 2024. PMID: 38282081 Free PMC article. Review.
-
Serum Bicarbonate Deficiency in Dogs with Acute and Chronic Kidney Disease.Vet Sci. 2023 May 19;10(5):363. doi: 10.3390/vetsci10050363. Vet Sci. 2023. PMID: 37235446 Free PMC article.
-
Efficacy and safety of oral sodium bicarbonate in kidney-transplant recipients and non-transplant patients with chronic kidney disease: a systematic review and meta-analysis.Front Pharmacol. 2024 Aug 26;15:1411933. doi: 10.3389/fphar.2024.1411933. eCollection 2024. Front Pharmacol. 2024. PMID: 39253380 Free PMC article.
-
Serum bicarbonate is associated with kidney outcomes in autosomal dominant polycystic kidney disease.Nephrol Dial Transplant. 2021 Dec 2;36(12):2248-2255. doi: 10.1093/ndt/gfaa283. Nephrol Dial Transplant. 2021. PMID: 33377160 Free PMC article.
-
Soft tissue calcifications in chronic kidney disease-beyond the vasculature.Pflugers Arch. 2025 Aug;477(8):1037-1059. doi: 10.1007/s00424-025-03098-0. Epub 2025 Jun 5. Pflugers Arch. 2025. PMID: 40471241 Free PMC article. Review.
References
-
- National Kidney Foundation : K/DOQI clinical practice guidelines for bone metabolism and disease in chronic kidney disease. Am J Kidney Dis 42[Suppl 3]: S1–S201, 2003 - PubMed
-
- Improving Global Outcomes (KDIGO) CKD Work Group : KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 3: 1–150, 2013
-
- Dobre M, Yang W, Chen J, Drawz P, Hamm LL, Horwitz E, Hostetter T, Jaar B, Lora CM, Nessel L, Ojo A, Scialla J, Steigerwalt S, Teal V, Wolf M, Rahman M; CRIC Investigators : Association of serum bicarbonate with risk of renal and cardiovascular outcomes in CKD: A report from the Chronic Renal Insufficiency Cohort (CRIC) study. Am J Kidney Dis 62: 670–678, 2013 - PMC - PubMed
-
- Menon V, Tighiouart H, Vaughn NS, Beck GJ, Kusek JW, Collins AJ, Greene T, Sarnak MJ: Serum bicarbonate and long-term outcomes in CKD. Am J Kidney Dis 56: 907–914, 2010 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
