

Formal guidelines: management of acute respiratory distress syndrome
- PMID: 31197492
- PMCID: PMC6565761
- DOI: 10.1186/s13613-019-0540-9
Formal guidelines: management of acute respiratory distress syndrome
Abstract
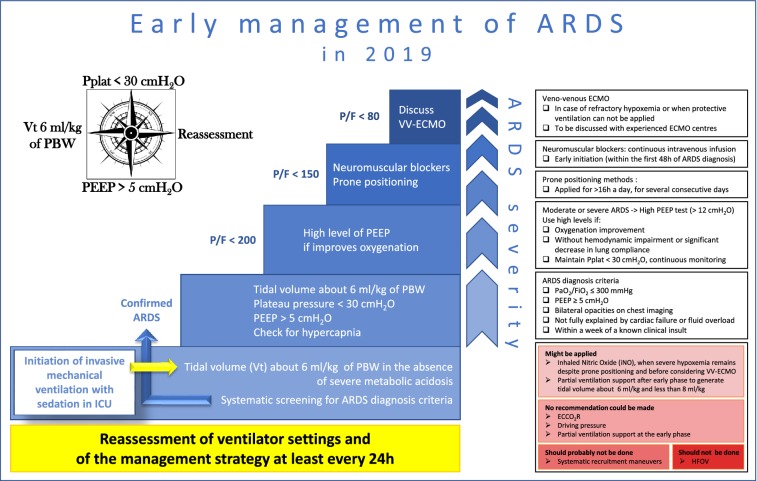
Fifteen recommendations and a therapeutic algorithm regarding the management of acute respiratory distress syndrome (ARDS) at the early phase in adults are proposed. The Grade of Recommendation Assessment, Development and Evaluation (GRADE) methodology has been followed. Four recommendations (low tidal volume, plateau pressure limitation, no oscillatory ventilation, and prone position) had a high level of proof (GRADE 1 + or 1 -); four (high positive end-expiratory pressure [PEEP] in moderate and severe ARDS, muscle relaxants, recruitment maneuvers, and venovenous extracorporeal membrane oxygenation [ECMO]) a low level of proof (GRADE 2 + or 2 -); seven (surveillance, tidal volume for non ARDS mechanically ventilated patients, tidal volume limitation in the presence of low plateau pressure, PEEP > 5 cmH2O, high PEEP in the absence of deleterious effect, pressure mode allowing spontaneous ventilation after the acute phase, and nitric oxide) corresponded to a level of proof that did not allow use of the GRADE classification and were expert opinions. Lastly, for three aspects of ARDS management (driving pressure, early spontaneous ventilation, and extracorporeal carbon dioxide removal), the experts concluded that no sound recommendation was possible given current knowledge. The recommendations and the therapeutic algorithm were approved by the experts with strong agreement.
Conflict of interest statement
Laurent Brochard: Philips; General Electric; Fisher Paykel; Air Liquide; Sentec; Medtronic Covidien. Jean-Daniel Chiche: General Electric Healthcare. Alain Combes: Maquet Getinge; Baxter. Samir Jaber: Drager; Fisher Paykel; Xenios. Armand Mekontso-Dessap: Air Liquide; Baxter; Fischer Paykel; Philips. Laurent Papazian: Air Liquide MS; MSD; Drager; Maquet; Medtronic. Jean-Christophe M. Richard: Air Liquide Medical System; Vygon; Covidien; General Electric. Damien Roux: Astellas. Antoine Vieillard-Baron: GSK. The remaining authors declare no competing interests.
Figures
References
-
- Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, Fan E, et al. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526–2533. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
