

Effectiveness of telemedicine systems for adults with heart failure: a meta-analysis of randomized controlled trials
- PMID: 31197564
- PMCID: PMC7046570
- DOI: 10.1007/s10741-019-09801-5
Effectiveness of telemedicine systems for adults with heart failure: a meta-analysis of randomized controlled trials
Abstract
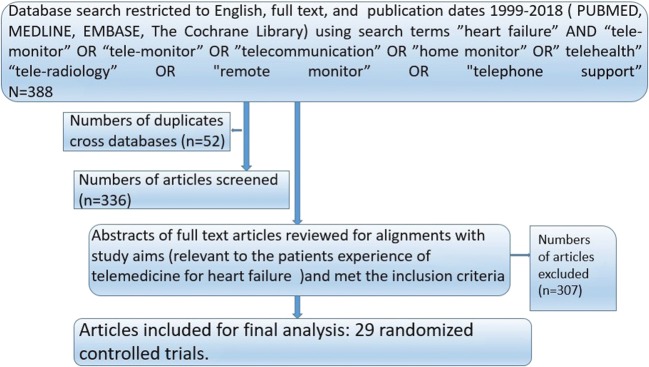
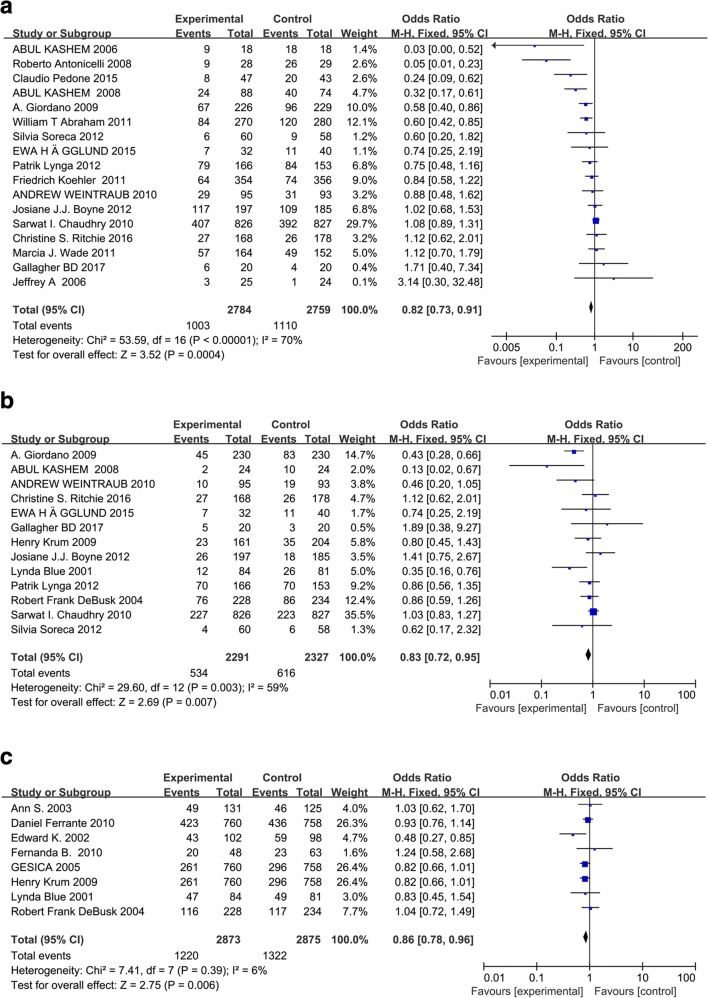
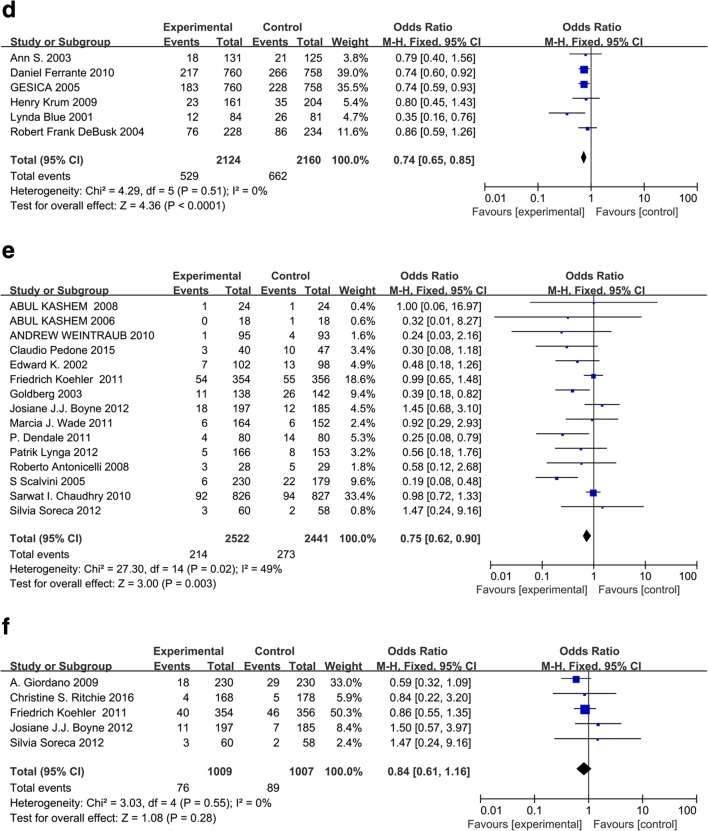
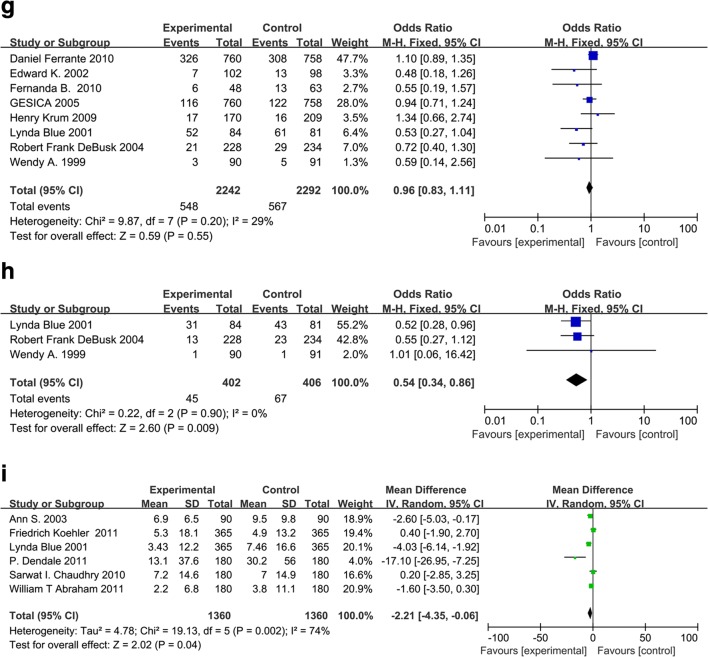
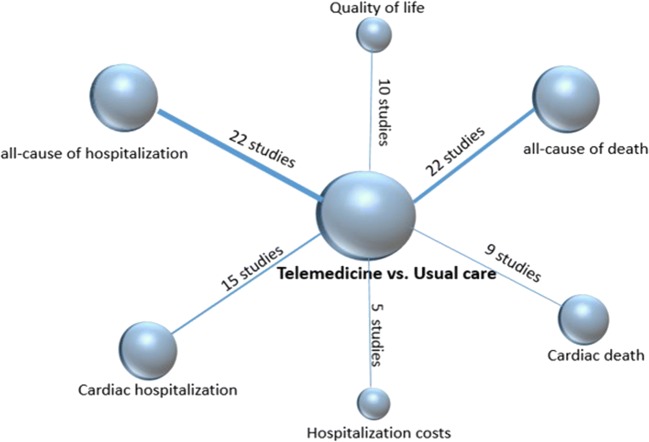
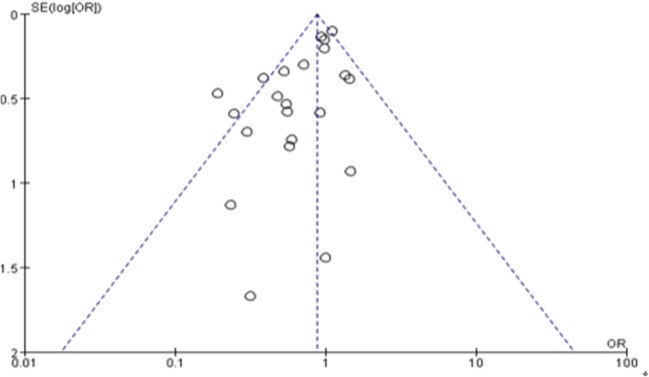
Despite favorable effects from telemedicine (TM) on cardiovascular diseases, outcome and comparative impact of TM on heart failure (HF) adults remain controversial. A meta-analysis was conducted to summarize the evidence from existing randomized controlled trials (RCTs) which compared potential impact of TM on HF with conventional healthcare. TM mainly included structure telephone support (STS), involving interactive vocal response monitoring and telemonitoring. PubMed, MEDLINE, EMBASE, and the Cochrane Library were searched to identify RCTs to fit our analysis (1999 to 2018). Odds ratio (OR) with its 95% confidence interval (CI) was used. Sensitivity analysis, subgroup analysis, and tests for publication bias were conducted. Heterogeneities were also evaluated by I2 tests. A total of 29 RCTs consisting of 10,981 HF adults were selected for meta-level synthesis, with follow-up range of 1-36 months. Telemonitoring is associated with the reduction in total number of all-cause hospitalization (OR 0.82, 95% CI 0.73-0.91, P = 0.0004) and cardiac hospitalization (OR 0.83, 95% CI 0.72-0.95, P = 0.007). Telemonitoring resulted in statistically significant risk reduction of all-cause mortality (OR 0.75, 95% CI 0.62-0.90, P = 0.003). However, the OR of HF-related mortality (OR 0.84, 95% CI 0.61-1.16, P = 0.28) is not significantly distinguishable from that of conventional healthcare. Receiving STS interventions is likely to reduce the hospitalization for all causes (OR 0.86, 95% CI 0.78-0.96, P = 0.006, I2 = 6%) and the hospitalization due to HF (OR 0.74, 95% CI 0.65-0.85, P < 0.0001, I2 = 0%), compared with interventions from conventional healthcare. OR of all-cause STS mortality (OR 0.96, 95% CI 0.83-1.11, P = 0.55) was identified in meta-analyses of eight cases. OR of STS cardiac mortality (OR 0.54, 95% CI 0.34-0.86, P = 0.009) was identified in meta-analyses of three cases. This work represents the comprehensive application of network meta-analysis to examine the comparative effectiveness of telemedicine interventions in improving HF patient outcomes. Compared with conventional healthcare, telemedicine systems with medical support prove to be more effective for HF adults, particularly in reducing all-cause hospitalization, cardiac hospitalization, all-cause mortality, cardiac mortality, and length of stay. While further research is required to confirm these observational findings and identify optimal telemedicine strategies and the duration of follow-up for which it confers benefits.
Keywords: Cardiovascular disease; Heart failure; Meta-analysis; Randomized controlled trials; Telemedicine.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
Similar articles
-
Which components of heart failure programmes are effective? A systematic review and meta-analysis of the outcomes of structured telephone support or telemonitoring as the primary component of chronic heart failure management in 8323 patients: Abridged Cochrane Review.Eur J Heart Fail. 2011 Sep;13(9):1028-40. doi: 10.1093/eurjhf/hfr039. Epub 2011 Jul 6. Eur J Heart Fail. 2011. PMID: 21733889
-
Remote monitoring of implantable cardiac devices in heart failure patients: a systematic review and meta-analysis of randomized controlled trials.Heart Fail Rev. 2020 May;25(3):469-479. doi: 10.1007/s10741-020-09923-1. Heart Fail Rev. 2020. PMID: 32002732
-
Comparative Effectiveness of Telemonitoring Versus Usual Care for Heart Failure: A Systematic Review and Meta-analysis.J Card Fail. 2018 Jan;24(1):19-28. doi: 10.1016/j.cardfail.2017.09.006. Epub 2017 Sep 20. J Card Fail. 2018. PMID: 28939459
-
Comparative Effectiveness of Disease Management With Information Communication Technology for Preventing Hospitalization and Readmission in Adults With Chronic Congestive Heart Failure.J Am Med Dir Assoc. 2018 Jun;19(6):472-479. doi: 10.1016/j.jamda.2018.03.012. Epub 2018 May 3. J Am Med Dir Assoc. 2018. PMID: 29730178
-
Effects of nurse-led transitional care interventions for patients with heart failure on healthcare utilization: A meta-analysis of randomized controlled trials.PLoS One. 2021 Dec 16;16(12):e0261300. doi: 10.1371/journal.pone.0261300. eCollection 2021. PLoS One. 2021. PMID: 34914810 Free PMC article.
Cited by
-
Rationale and design of the AMULET study: A new Model of telemedical care in patients with heart failure.ESC Heart Fail. 2021 Aug;8(4):2569-2579. doi: 10.1002/ehf2.13330. Epub 2021 Apr 22. ESC Heart Fail. 2021. PMID: 33887120 Free PMC article. Clinical Trial.
-
VPExam Virtual Care for Heart Failure Optimizing Transitions of Care Quality Improvement Project (VPExam QI).Cardiovasc Digit Health J. 2022 May 11;3(3):146-155. doi: 10.1016/j.cvdhj.2022.04.002. eCollection 2022 Jun. Cardiovasc Digit Health J. 2022. PMID: 35720679 Free PMC article. No abstract available.
-
Experiences and Perceptions of Patients and Providers Participating in Remote Titration of Heart Failure Medication Facilitated by Telemonitoring: Qualitative Study.JMIR Cardio. 2021 Nov 25;5(2):e28259. doi: 10.2196/28259. JMIR Cardio. 2021. PMID: 34842546 Free PMC article.
-
Telemedicine and patients with heart failure: evidence and unresolved issues.Einstein (Sao Paulo). 2024 Mar 4;22:eRW0393. doi: 10.31744/einstein_journal/2024RW0393. eCollection 2024. Einstein (Sao Paulo). 2024. PMID: 38451690 Free PMC article. Review.
-
Interactive Remote Patient Monitoring Devices for Managing Chronic Health Conditions: Systematic Review and Meta-analysis.J Med Internet Res. 2022 Nov 3;24(11):e35508. doi: 10.2196/35508. J Med Internet Res. 2022. PMID: 36326818 Free PMC article.
References
-
- Pandor A, Gomersall T, Stevens JW, Wang J, Al-Mohammad A, Bakhai A, Cleland JG, Cowie MR, Wong R. Remote monitoring after recent hospital discharge in patients with heart failure: a systematic review and network meta-analysis. Heart. 2013;99(23):1717–1726. doi: 10.1136/heartjnl-2013-303811. - DOI - PubMed
-
- Koehler F, Winkler S, Schieber M, Sechtem U, Stangl K, Bohm M, de Brouwer S, Perrin E, Baumann G, Gelbrich G, Boll H, Honold M, Koehler K, Kirwan BA, Anker SD. Telemedicine in heart failure: pre-specified and exploratory subgroup analyses from the TIM-HF trial. Int J Cardiol. 2012;161(3):143–150. doi: 10.1016/j.ijcard.2011.09.007. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
