

Effect of sodium-glucose cotransporter 2 inhibitor on proximal tubular function and injury in patients with type 2 diabetes: a randomized controlled trial
- PMID: 31198224
- PMCID: PMC6543969
- DOI: 10.1093/ckj/sfy122
Effect of sodium-glucose cotransporter 2 inhibitor on proximal tubular function and injury in patients with type 2 diabetes: a randomized controlled trial
Abstract
Background: Intensive glucose control reduces the risk for microvascular complications in type 2 diabetes (T2DM). Recently, sodium-glucose cotransporter 2 (SGLT2) inhibitors have been shown to exert renoprotection beyond glycemic control, although their effects on the organs are not well known. There are limited data on SGLT2 inhibitors for the biomarkers of kidney injury in type 2 diabetes mellitus (T2DM) patients.
Objective: Our objective was to demonstrate the effect of SGLT2 inhibitors on proximal tubular injury and function in patients with T2DM.
Methods: T2DM patients with persistent glycated hemoglobin (HbA1c) levels >7% were randomly assigned to either dapagliflozin 10 mg/day (n = 28) or standard treatment (n = 29) for 12 weeks. Proximal tubular injury biomarkers, including urine kidney injury molecule-1:creatinine ratio (UKIM1CR), urine cystatin C:creatinine ratio (UCCR), urine albumin:creatinine ratio (UACR), fractional excretion of phosphate (FEPO4) and fractional excretion of uric acid (FEUA) were measured at baseline and study end.
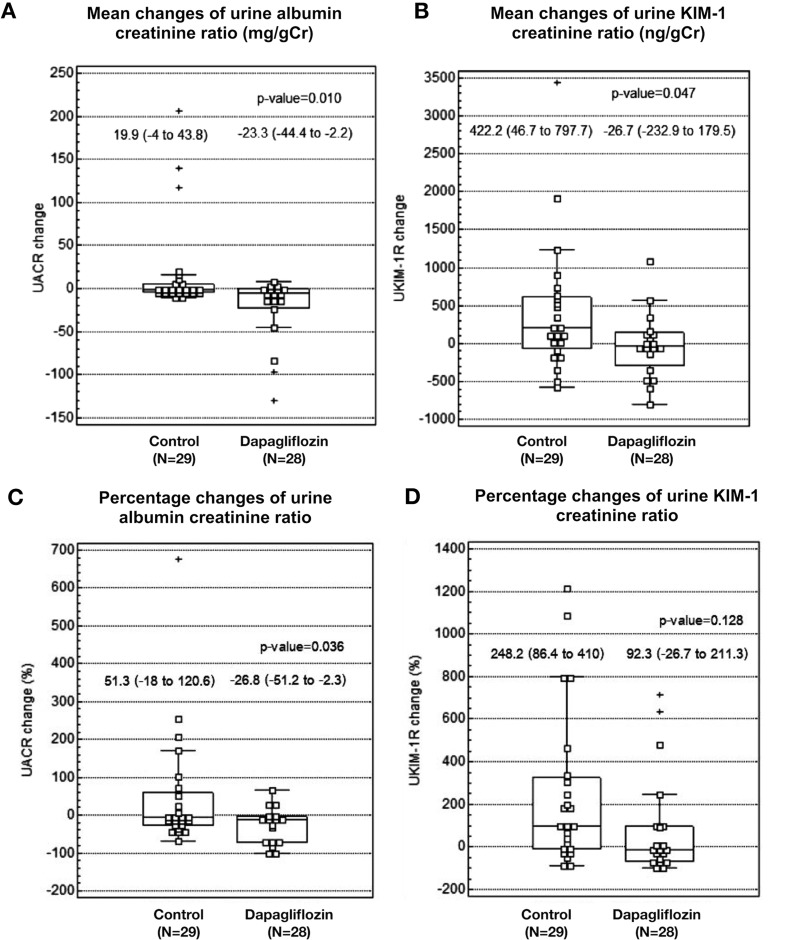
Results: Baseline characteristics were comparable between treatment groups. After 12 weeks, dapagliflozin-treated versus standard-treated patients showed reductions in HbA1c (-0.75 ± 0.21 versus -0.70 ± 0.25%; P = 0.882). There were significant between-group differences in the reduction in UACR {-23.3 [95% confidence interval (CI) -44.4 to -2.2] versus +19.9 (-4.0-43.8) mg/g Cr; P = 0.010} and UKIM1CR [-26.7 (95% CI -232.9-179.5) versus +422.2 (46.7-797.7) ng/g Cr; P = 0.047], but no significant difference in changes in UCCR between the two groups. There was no significant change in glomerular filtration rate, serum phosphate level, FEUA and FEPO4 in the dapagliflozin group. No serious renal-related adverse events were observed in either group.
Conclusions: This study indicates that dapagliflozin in T2DM patients can decrease the levels of urinary proximal tubular injury biomarkers, thus highlighting its renoprotective effect. SGLT2 inhibitors could prove useful in treating T2DM by protecting against renal tubular injury and may lead to reduced long-term renal outcomes.
Keywords: cystatin C; dapagliflozin; kidney injury molecule-1; sodium-glucose cotransporter 2 inhibitor; type 2 diabetes.
Figures
Similar articles
-
Albuminuria and Serum Tumor Necrosis Factor Receptor Levels in Patients with Type 2 Diabetes on SGLT2 Inhibitors: A Prospective Study.Diabetes Ther. 2024 Jan;15(1):127-143. doi: 10.1007/s13300-023-01488-0. Epub 2023 Oct 26. Diabetes Ther. 2024. PMID: 37883001 Free PMC article.
-
Renoprotective Effects of Additional SGLT2 inhibitor Therapy in Patients With Type 2 Diabetes Mellitus and Chronic Kidney Disease Stages 3b-4: A Real World Report From A Japanese Specialized Diabetes Care Center.J Clin Med Res. 2019 Apr;11(4):267-274. doi: 10.14740/jocmr3761. Epub 2019 Mar 18. J Clin Med Res. 2019. PMID: 30937117 Free PMC article.
-
Effect of dapagliflozin on urinary albumin excretion in patients with chronic kidney disease with and without type 2 diabetes: a prespecified analysis from the DAPA-CKD trial.Lancet Diabetes Endocrinol. 2021 Nov;9(11):755-766. doi: 10.1016/S2213-8587(21)00243-6. Epub 2021 Oct 4. Lancet Diabetes Endocrinol. 2021. PMID: 34619106 Clinical Trial.
-
Sodium Glucose Cotransporter 2 Inhibitors in the Treatment of Diabetes Mellitus: Cardiovascular and Kidney Effects, Potential Mechanisms, and Clinical Applications.Circulation. 2016 Sep 6;134(10):752-72. doi: 10.1161/CIRCULATIONAHA.116.021887. Epub 2016 Jul 28. Circulation. 2016. PMID: 27470878 Review.
-
Plausible prediction of renoprotective effects of sodium-glucose cotransporter-2 inhibitors in patients with chronic kidney diseases.J Int Med Res. 2024 Feb;52(2):3000605241227659. doi: 10.1177/03000605241227659. J Int Med Res. 2024. PMID: 38329077 Free PMC article. Review.
Cited by
-
Sodium-Glucose Transporter 2 (SGLT2) Inhibitors and Iron Deficiency in Heart Failure and Chronic Kidney Disease: A Literature Review.Life (Basel). 2023 Dec 13;13(12):2338. doi: 10.3390/life13122338. Life (Basel). 2023. PMID: 38137939 Free PMC article. Review.
-
Mechanisms of action of the sodium-glucose cotransporter-2 (SGLT2) inhibitor canagliflozin on tubular inflammation and damage: A post hoc mediation analysis of the CANVAS trial.Diabetes Obes Metab. 2022 Oct;24(10):1950-1956. doi: 10.1111/dom.14779. Epub 2022 Jun 28. Diabetes Obes Metab. 2022. PMID: 35635326 Free PMC article. Clinical Trial.
-
Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation and Study of Diabetic Nephropathy with Atrasentan: what was learned about the treatment of diabetic kidney disease with canagliflozin and atrasentan?Clin Kidney J. 2019 May 31;12(3):313-321. doi: 10.1093/ckj/sfz070. eCollection 2019 Jun. Clin Kidney J. 2019. PMID: 31198532 Free PMC article.
-
Effects of SGLT2 Inhibitors on Kidney and Cardiovascular Function.Annu Rev Physiol. 2021 Feb 10;83:503-528. doi: 10.1146/annurev-physiol-031620-095920. Epub 2020 Nov 16. Annu Rev Physiol. 2021. PMID: 33197224 Free PMC article. Review.
-
The Pathophysiological Basis of Diabetic Kidney Protection by Inhibition of SGLT2 and SGLT1.Kidney Dial. 2022 Jun;2(2):349-368. doi: 10.3390/kidneydial2020032. Epub 2022 Jun 18. Kidney Dial. 2022. PMID: 36380914 Free PMC article.
References
-
- Goff DC Jr, Gerstein HC, Ginsberg HN. et al. Prevention of cardiovascular disease in persons with type 2 diabetes mellitus: current knowledge and rationale for the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial. Am J Cardiol 2007; 99: 4i–20i - PubMed
-
- Ingsathit A., Thakkinstian A, Chaiprasert P. et al. Prevalence and risk factors of chronic kidney disease in the Thai adult population: Thai SEEK study. Nephrol Dial Transplant 2010; 25: 1567–1575 - PubMed
-
- Satirapoj B, Supasyndh O, Mayteedol N. et al. Metabolic syndrome and its relation to chronic kidney disease in a Southeast Asian population. Southeast Asian J Trop Med Public Health 2011; 42: 176–183 - PubMed
-
- Satirapoj B. Review on pathophysiology and treatment of diabetic kidney disease. J Med Assoc Thai 2010; 93(Suppl 6): S228–S241 - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
