

Antibiotic-resistant hypervirulent Klebsiella pneumoniae causing community- acquired liver abscess: an emerging disease
- PMID: 31198568
- PMCID: PMC6544431
- DOI: 10.1093/omcr/omz032
Antibiotic-resistant hypervirulent Klebsiella pneumoniae causing community- acquired liver abscess: an emerging disease
Abstract
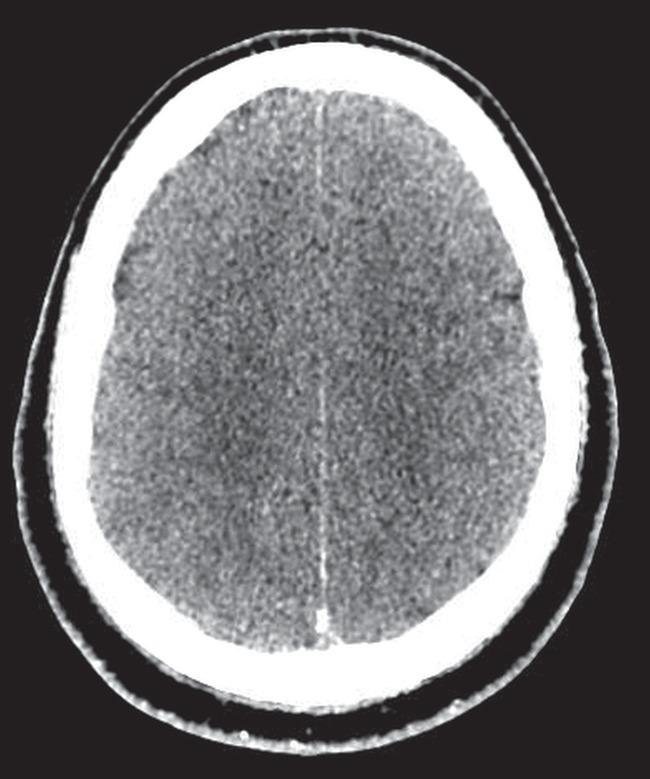
We report a case of a patient with fatal community-acquired pyogenic liver abscess (CA-PLA) caused by multi drug-resistant, hypervirulent, Klebsiella pneumoniae (mdrhvKP). HvKP causing PLA has been described in East and South East Asia and it is recognized as an emerging infection worldwide. The syndrome is characterized by cryptogenic liver abscess formation without a previous history of hepatobiliary or colonic disease and metastatic spread of infection via the bloodstream to distant sites, including lungs, central nervous system and other organ systems. Diabetes mellitus is a recognized risk factor. Most previously reported cases have involved antibiotic susceptible strains of hvKP although reports of bloodstream infections caused by resistant strains, including carbapenemase producers, are increasing. Our report highlights the need for awareness of this devastating infection in patients presenting with sepsis and liver abscess without underlying hepatobiliary or colonic disease.
Figures








References
-
- Siu LK, Yeh KM, Lin JC, Fung CP, Chang FY. Klebsiella pneumoniae liver abscess: a new invasive syndrome. Lancet Infect Dis 2012;12:881–887. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
