

Analysis of dementia in the US population using Medicare claims: Insights from linked survey and administrative claims data
- PMID: 31198838
- PMCID: PMC6556828
- DOI: 10.1016/j.trci.2019.04.003
Analysis of dementia in the US population using Medicare claims: Insights from linked survey and administrative claims data
Abstract
Introduction: Medicare claims data may be a rich data source for tracking population dementia rates. Insufficient understanding of completeness of diagnosis, and for whom, limits their use.
Methods: We analyzed agreement in prevalent and incident dementia based on cognitive assessment from the Health and Retirement Study for persons with linked Medicare claims from 2000 to 2008 (N = 10,450 persons). Multinomial logistic regression identified sociodemographic factors associated with disagreement.
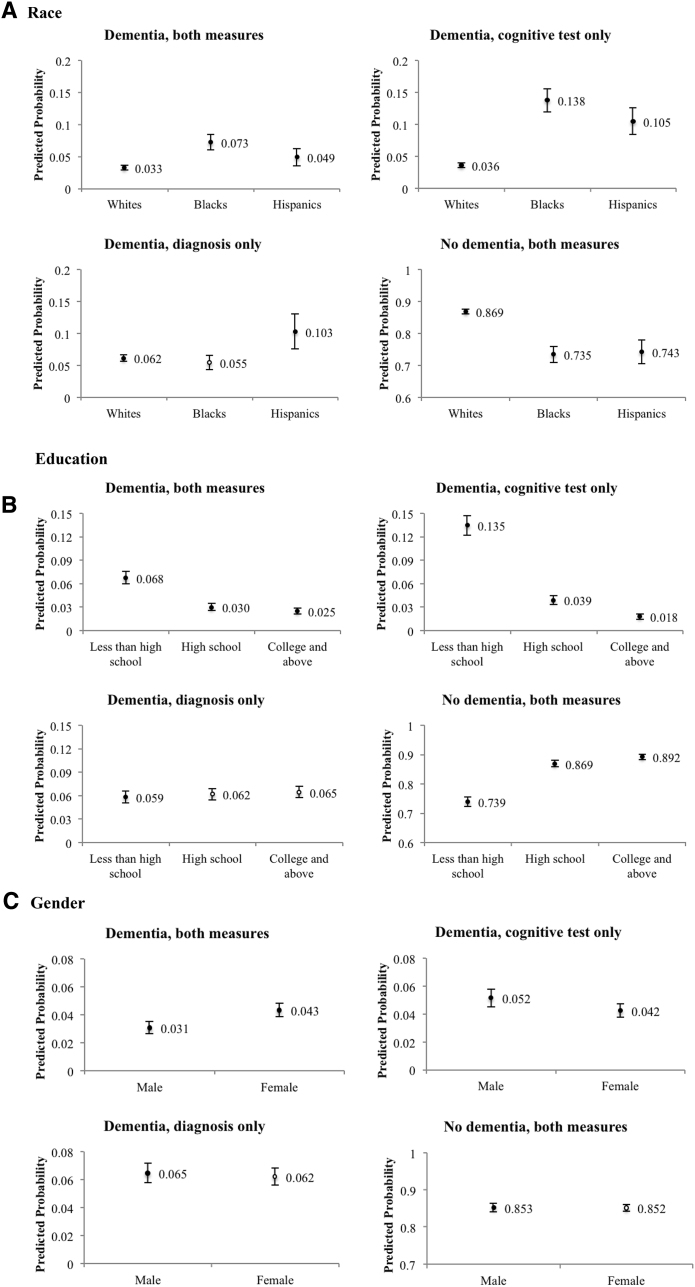
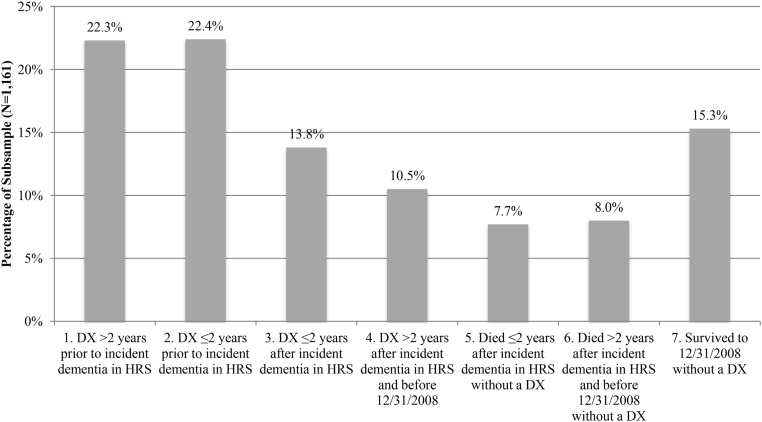
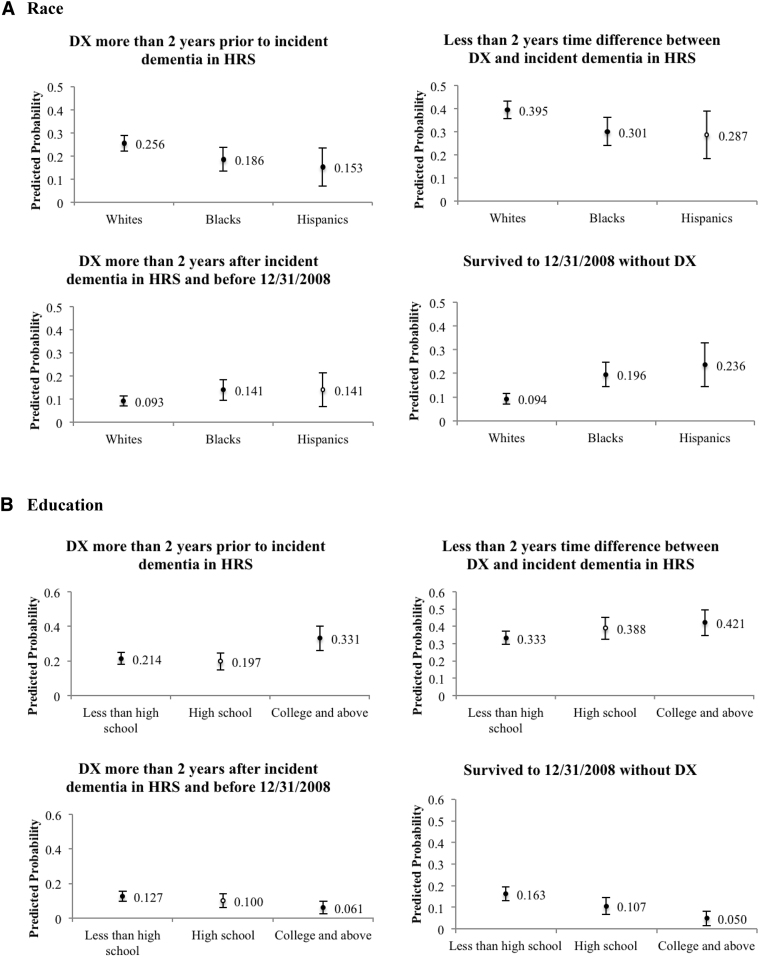
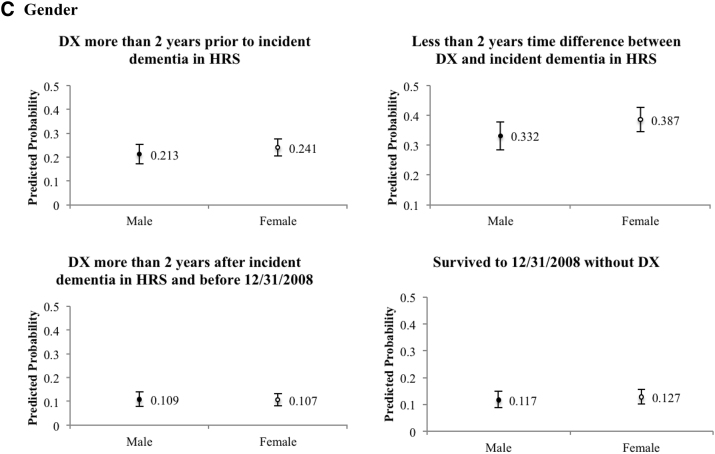
Results: Survey-based cognitive tests and claims-based dementia diagnosis yielded equal prevalence estimates, yet only half were identified by both measures. Race and education were associated with disagreement. Eighty-five percent of respondents with incident dementia measured by cognitive decline received a diagnosis or died within the study period, with lower odds among blacks and Hispanics than among whites.
Discussions: Claims data are valuable for tracking dementia in the US population and improve over time. Delayed diagnosis may underestimate rates within black and Hispanic populations.
Keywords: Cognition; Diagnosis; Disparities; Incidence; Prevalence; Race/ethnicity.
Figures
References
-
- Valcour V.G., Masaki K.H., Curb J.D., Blanchette P.L. The detection of dementia in the primary care setting. Arch Intern Med. 2000;160:2964–2968. - PubMed
-
- Chodosh J., Petitti D.B., Elliott M., Hays R.D., Crooks V.C., Reuben D.B. Physician recognition of cognitive impairment: evaluating the need for improvement. J Am Geriatr Soc. 2004;52:1051–1059. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources