

Association of Undifferentiated Dyspnea in Late Life With Cardiovascular and Noncardiovascular Dysfunction: A Cross-sectional Analysis From the ARIC Study
- PMID: 31199443
- PMCID: PMC6575149
- DOI: 10.1001/jamanetworkopen.2019.5321
Association of Undifferentiated Dyspnea in Late Life With Cardiovascular and Noncardiovascular Dysfunction: A Cross-sectional Analysis From the ARIC Study
Abstract
Importance: Undifferentiated dyspnea is common in late life, but the relative contribution of subclinical cardiac dysfunction is unknown. Impairments in cardiac structure and function may be characteristics of undifferentiated dyspnea in elderly people, providing potential insights into occult heart failure (HF).
Objective: To quantify the association of undifferentiated dyspnea with cardiac dysfunction after accounting for other potential contributors.
Design, setting, and participants: This cross-sectional study used data from Atherosclerosis Risk in Communities study participants 65 years and older who attended the fifth study visit (from 2011 to 2013) and had not been diagnosed with HF, chronic obstructive pulmonary disease, morbid obesity, or severe kidney disease. Analyses were conducted from October 2017 to June 2018.
Exposures: Dyspnea measured using the modified Medical Research Council scale, with a score less than 2 classified as none to mild and a score of 2 or more classified as moderate to severe.
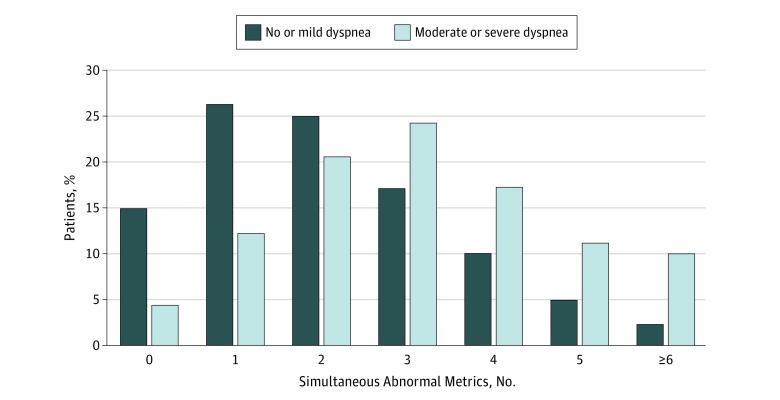
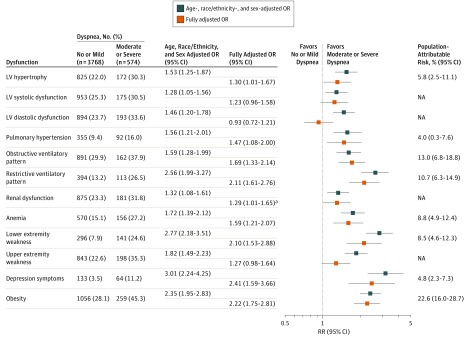
Main outcomes and measures: Using multivariable logistic regression, the association of undifferentiated dyspnea was defined using cardiac structure, systolic and diastolic function, pulmonary pressure (echocardiography), pulmonary function (spirometry), glomerular filtration rate, hemoglobin, body mass index, depression, and physical performance. The population-attributable risk was calculated for each dysfunction metric.
Results: Among 4342 participants (mean [SD] age, 75.9 [5.0] years; 2533 [58.3%] women), 1173 (27.0%) had undifferentiated dyspnea. Moderate to severe dyspnea was present in 574 participants (13.2%) and was associated with left ventricular (LV) hypertrophy (odds ratio [OR], 1.53; 95% CI, 1.25-1.87; P < .001) and LV diastolic (OR, 1.46; 95% CI, 1.20-1.78; P < .001) and systolic (OR, 1.28; 95% CI, 1.05-1.56; P = .02) dysfunction. Moderate to severe dyspnea was also associated with obstructive (OR, 1.59; 95% CI, 1.28-1.99; P < .001) and restrictive (OR, 2.56; 95% CI, 1.99-3.27; P < .001) findings on spirometry, renal impairment (OR, 1.32; 95% CI, 1.08-1.61; P = .01), anemia (OR, 1.72; 95% CI, 1.39-2.12; P < .001), lower (OR, 2.77; 95% CI, 2.18-3.51; P < .001) and upper (OR, 1.82; 95% CI, 1.49-2.23; P < .001) extremity weakness, depression (OR, 3.01; 95% CI, 2.24-4.25; P < .001), and obesity (OR, 2.35; 95% CI, 1.95-2.83; P < .001). After accounting for these, moderate to severe dyspnea was associated with LV hypertrophy (OR, 1.30; 95% CI, 1.01-1.67; P = .04) and was not associated with systolic or diastolic function. In contrast, in the fully adjusted model, other organ system measures were associated with dyspnea, except for glomerular filtration rate and grip strength. The population-attributable risk of dyspnea associated with obesity alone was 22.6% compared with 5.8% for LV hypertrophy.
Conclusions and relevance: Undifferentiated dyspnea is multifactorial in older adults, and this study showed an association with obesity. When accounting for other relevant organ systems, cardiovascular function poorly discriminated those with vs those without dyspnea. Therefore, dyspnea should not be assumed to represent occult HF in this population.
Conflict of interest statement
Figures
References
-
- Santos M, Kitzman DW, Matsushita K, Loehr L, Sueta CA, Shah AM. Prognostic importance of dyspnea for cardiovascular outcomes and mortality in persons without prevalent cardiopulmonary disease: the Atherosclerosis Risk in Communities study. PLoS One. 2016;11(10):e0165111. doi: 10.1371/journal.pone.0165111 - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
