

Progressive agrammatic aphasia without apraxia of speech as a distinct syndrome
- PMID: 31199471
- PMCID: PMC6658844
- DOI: 10.1093/brain/awz157
Progressive agrammatic aphasia without apraxia of speech as a distinct syndrome
Abstract
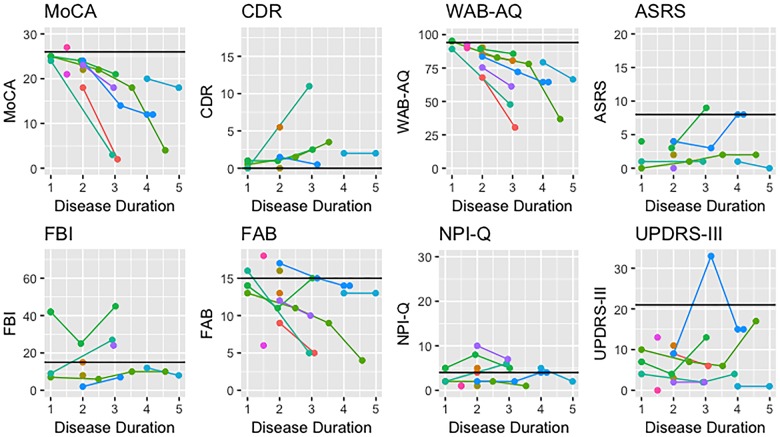
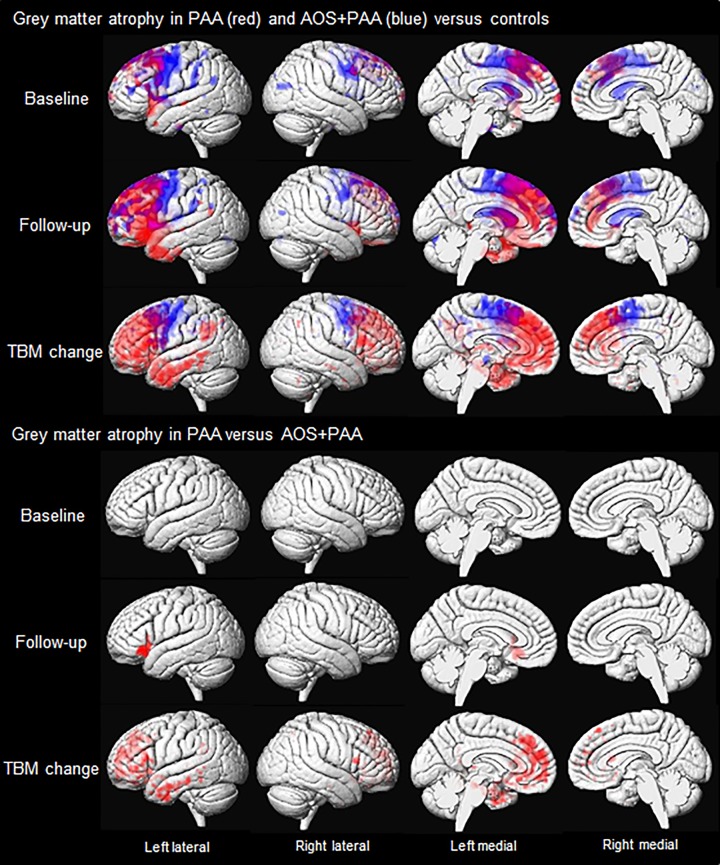
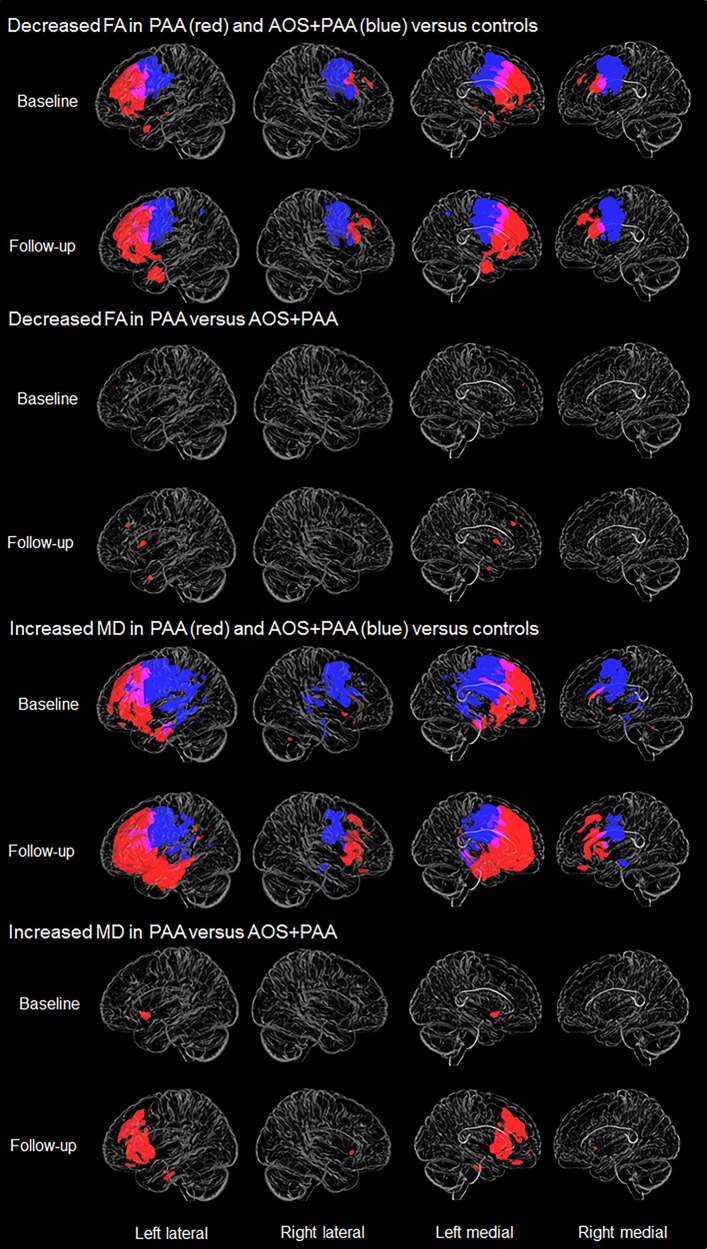
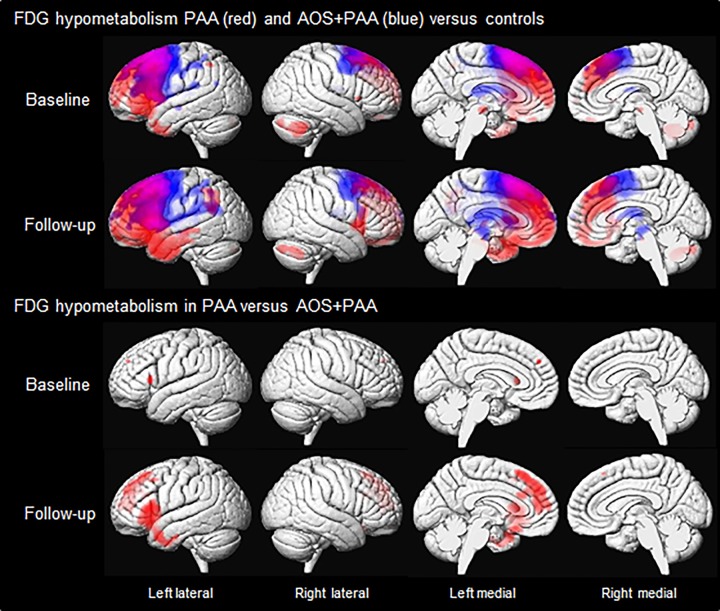
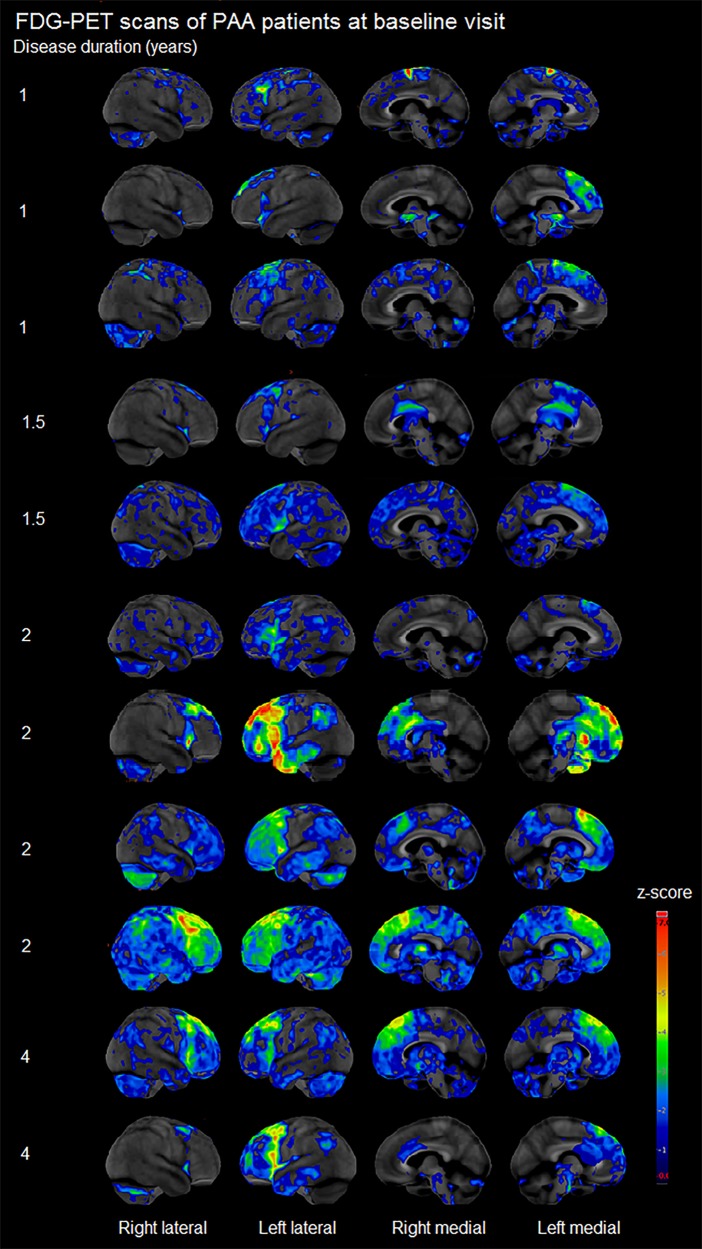
Agrammatic aphasia affects grammatical language production and can result from a neurodegenerative disease. Although it typically presents with concomitant apraxia of speech, this is not always the case. Little is known about the clinical course and imaging features of patients that present with agrammatism in the absence of apraxia of speech, which we will refer to as progressive agrammatic aphasia. We aimed to make a detailed description of the longitudinal clinical, linguistic, and neuroimaging features of a cohort of 11 patients with progressive agrammatic aphasia to provide a complete picture of this syndrome. All patients underwent detailed speech and language, neurological and neuropsychological assessments, 3 T structural and diffusion tensor imaging MRI, 18F-fluorodeoxyglucose and Pittsburgh compound B PET. The 11 patients were matched by age and gender to 22 patients who had mixed apraxia of speech and agrammatism. The progressive agrammatic aphasia patients performed abnormally on tests of language, general cognition, executive function, and functional ability at baseline and declined in these measures over time. Only two patients eventually developed apraxia of speech, while parkinsonism was absent-to-mild throughout all visits for all patients. When compared to the patients with mixed apraxia of speech and agrammatism, the patients with progressive agrammatic aphasia performed better on tests of motor speech and parkinsonism but more poorly, and declined faster over time, on tests of general aphasia severity, agrammatism, and naming. The patients with progressive agrammatic aphasia also showed different neuroimaging abnormalities, with greater atrophy, hypometabolism and white matter tract degeneration in the prefrontal and anterior temporal lobes compared to patients with mixed apraxia of speech and agrammatism. These differences were more pronounced as the disease progressed. These results demonstrate that progressive agrammatic aphasia has a different clinical disease course and different underlying neuroanatomical abnormalities than patients with the more common syndrome of mixed agrammatism and apraxia of speech. This supports the distinction of progressive agrammatic aphasia and has implications for the classification of patients with agrammatic aphasia.
Keywords: MRI; agrammatic; aphasia; longitudinal; positron emission tomography.
© The Author(s) (2019). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
References
-
- Ashburner J, Barnes G, Chen C, Daunizeau J, Flandin G, Friston K et al. . SPM12 manual. London: Wellcome Trust Centre for Neuroimaging; 2014.
