

Current Challenges in Diagnosis and Assessment of the Response of Locally Advanced and Metastatic Renal Cell Carcinoma
- PMID: 31199711
- PMCID: PMC6677287
- DOI: 10.1148/rg.2019180178
Current Challenges in Diagnosis and Assessment of the Response of Locally Advanced and Metastatic Renal Cell Carcinoma
Abstract
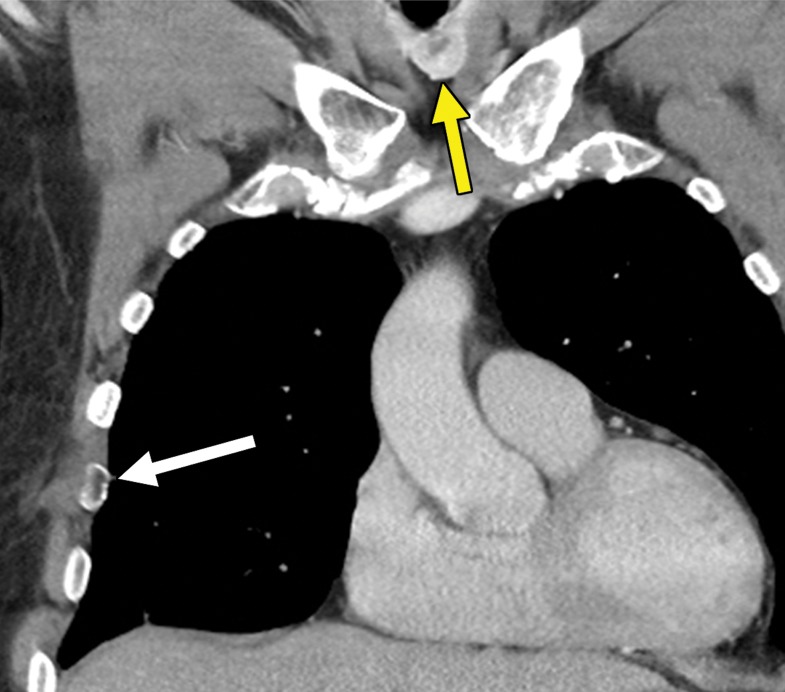
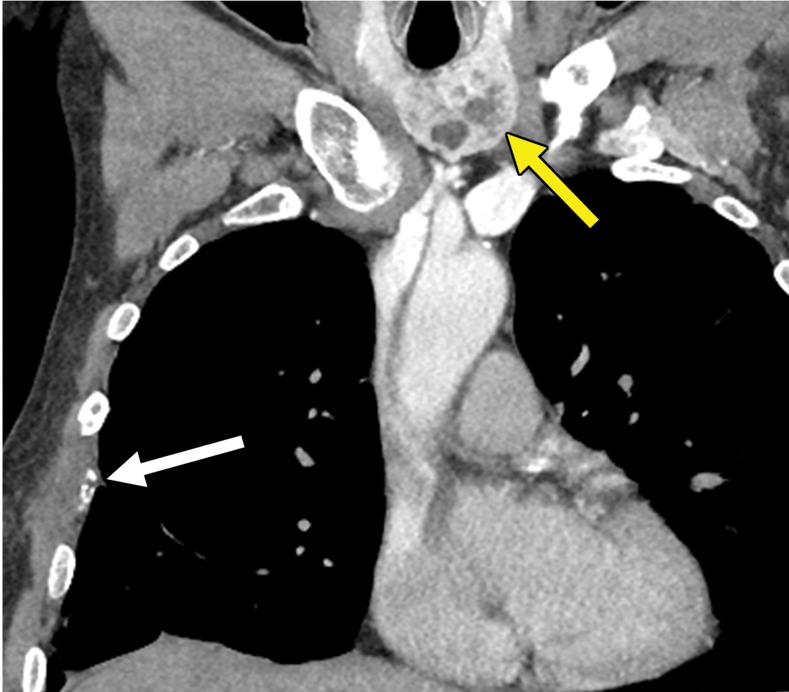
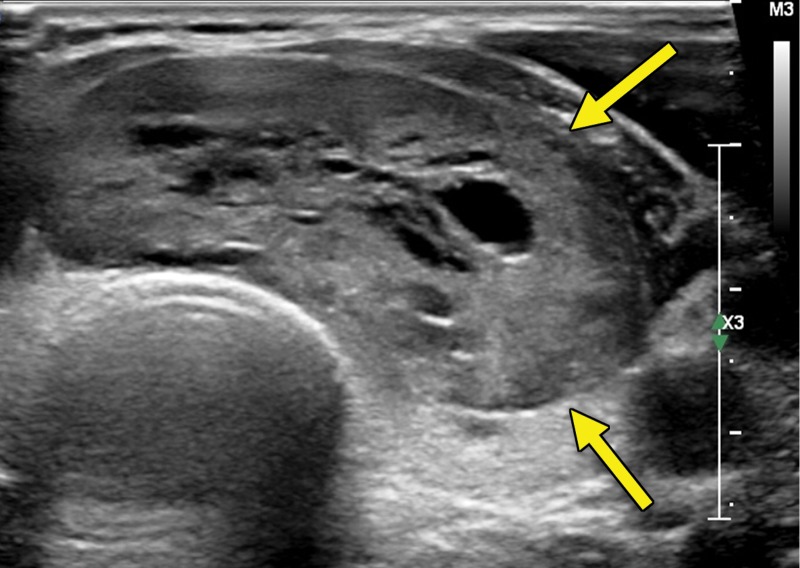
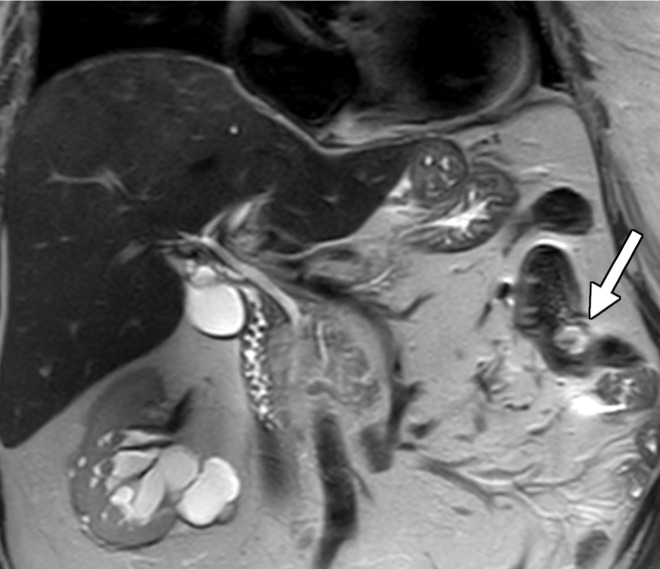
Locally advanced and metastatic renal cell carcinoma (RCC) present a specific set of challenges to the radiologist. The detection of metastatic disease is confounded by the ability of RCC to metastasize to virtually any part of the human body long after surgical resection of the primary tumor. This includes sites not commonly included in routine surveillance, which come to light after the patient becomes symptomatic. In the assessment of treatment response, the phenomenon of tumor heterogeneity, where clone selection through systemic therapy drives the growth of potentially more aggressive phenotypes, can result in oligoprogression despite overall disease control. Finally, advances in therapy have resulted in the development of immuno-oncologic agents that may result in changes that are not adequately evaluated with conventional size-based response criteria and may even be misinterpreted as progression. This article reviews the common challenges a radiologist may encounter in the evaluation of patients with locally advanced and metastatic RCC. ©RSNA, 2019.
Figures






Similar articles
-
[Local recurrence and metastatic dissemination of renal cell carcinoma: clinical and imaging characteristics].J Radiol. 2003 Mar;84(3):275-84. J Radiol. 2003. PMID: 12736586 Review. French.
-
Additional benefit of SPECT/CT in bone scanning of metastatic renal cell carcinoma.Clin Nucl Med. 2007 May;32(5):411-4. doi: 10.1097/01.rlu.0000259641.90922.1f. Clin Nucl Med. 2007. PMID: 17452879 No abstract available.
-
[Duodenal bleeding revealing a renal cell carcinoma].Gastroenterol Clin Biol. 2002 Nov;26(11):1044-6. Gastroenterol Clin Biol. 2002. PMID: 12483141 French.
-
Renal cell carcinoma metastatic to the pancreas: clinical and radiological features.Mayo Clin Proc. 2000 Jun;75(6):581-5. doi: 10.4065/75.6.581. Mayo Clin Proc. 2000. PMID: 10852418
-
Imaging in metastatic renal cell carcinoma.AJR Am J Roentgenol. 2007 Aug;189(2):360-70. doi: 10.2214/AJR.07.2077. AJR Am J Roentgenol. 2007. PMID: 17646462 Review.
Cited by
-
Second-Line Systemic Therapies in Metastatic Renal Cell Carcinoma: Current Insights and Future Directions.J Cancer Immunol (Wilmington). 2025;7(2):81-94. doi: 10.33696/cancerimmunol.7.107. J Cancer Immunol (Wilmington). 2025. PMID: 40661855 Free PMC article.
-
Secondary Breast Malignancy from Renal Cell Carcinoma: Challenges in Diagnosis and Treatment-Case Report.Diagnostics (Basel). 2023 Mar 5;13(5):991. doi: 10.3390/diagnostics13050991. Diagnostics (Basel). 2023. PMID: 36900135 Free PMC article.
-
Curcumin reverses the sunitinib resistance in clear cell renal cell carcinoma (ccRCC) through the induction of ferroptosis via the ADAMTS18 gene.Transl Cancer Res. 2021 Jul;10(7):3158-3167. doi: 10.21037/tcr-21-227. Transl Cancer Res. 2021. PMID: 35116623 Free PMC article.
-
Use of dual-energy CT for renal mass assessment.Eur Radiol. 2021 Jun;31(6):3721-3733. doi: 10.1007/s00330-020-07426-z. Epub 2020 Nov 18. Eur Radiol. 2021. PMID: 33210200 Review.
-
KIDNEY-PAGER: analysis of circulating tumor DNA as a biomarker in renal cancer - an observational trial. Study protocol.Acta Oncol. 2024 Feb 23;63:51-55. doi: 10.2340/1651-226X.2024.25581. Acta Oncol. 2024. PMID: 38391290 Free PMC article.
References
-
- Amin MB, Amin MB, Tamboli P, et al. . Prognostic impact of histologic subtyping of adult renal epithelial neoplasms: an experience of 405 cases. Am J Surg Pathol 2002;26(3):281–291. - PubMed
-
- Patard JJ, Leray E, Rioux-Leclercq N, et al. . Prognostic value of histologic subtypes in renal cell carcinoma: a multicenter experience. J Clin Oncol 2005;23(12):2763–2771. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin 2016;66(1):7–30. - PubMed
-
- Noone AMHN, Krapcho M, Miller D, et al. . SEER cancer statistics review, 1975-2015. Bethesda, Md: National Cancer Institute. https://seer.cancer.gov/csr/1975_2015/. Accessed April 20, 2018.
-
- Ross H, Martignoni G, Argani P. Renal cell carcinoma with clear cell and papillary features. Arch Pathol Lab Med 2012;136(4):391–399. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
