

Lymphocytopenia as a Predictor of Mortality in Patients with ICU-Acquired Pneumonia
- PMID: 31200458
- PMCID: PMC6617552
- DOI: 10.3390/jcm8060843
Lymphocytopenia as a Predictor of Mortality in Patients with ICU-Acquired Pneumonia
Abstract
Background: Intensive care unit-acquired pneumonia (ICU-AP) is a severe complication in patients admitted to the ICU. Lymphocytopenia is a marker of poor prognosis in patients with community-acquired pneumonia, but its impact on ICU-AP prognosis is unknown. We aimed to evaluate whether lymphocytopenia is an independent risk factor for mortality in non-immunocompromised patients with ICU-AP.
Methods: Prospective observational cohort study of patients from six ICUs of an 800-bed tertiary teaching hospital (2005 to 2016).
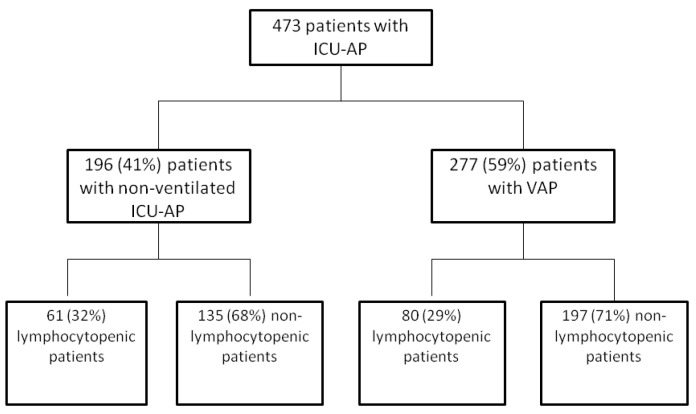
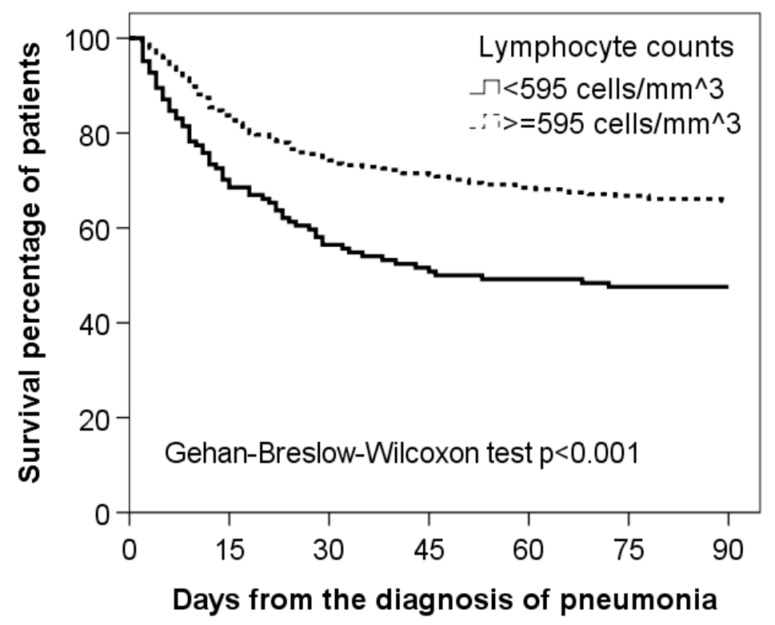
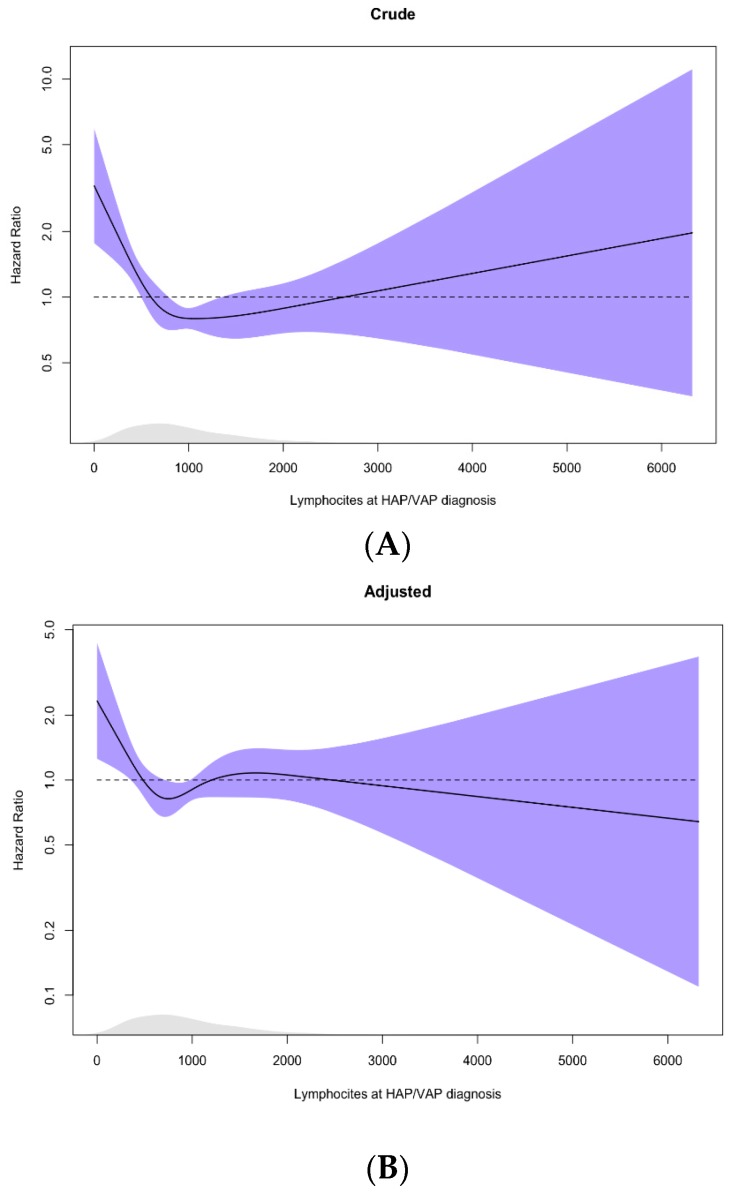
Results: Of the 473 patients included, 277 (59%) had ventilator-associated pneumonia (VAP). Receiver operating characteristic (ROC) analysis of the lymphocyte counts at diagnosis showed that 595 cells/mm3 was the best cut-off for discriminating two groups of patients at risk: lymphocytopenic group (lymphocyte count <595 cells/mm3, 141 patients (30%)) and non-lymphocytopenic group (lymphocyte count ≥595 cells/mm3, 332 patients (70%)). Patients with lymphocytopenia presented more comorbidities and a higher sequential organ failure assessment (SOFA) score at the moment of pneumonia diagnosis. Also, 28-day mortality and 90-day mortality were higher in patients with lymphocytopenia (28-day: 38 (27%) versus 59 (18%), 90-day: 74 (53%) versus 111 (34%)). In the multivariable model, <595 cells/mm3 resulted to be an independent predictor for 90-day mortality (Hazard Ratio 1.41; 95% Confidence Interval 1.02 to 1.94).
Conclusion: Lymphocytopenia is an independent predictor of 90-day mortality in non-immunocompromised patients with ICU-AP.
Keywords: host response; infection; intensive care unit-acquired pneumonia; lymphocytes; mortality.
Conflict of interest statement
The authors have no conflicts of interest to declare. The funding sources had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Figures
References
-
- Magill S.S., Edwards J.R., Bamberg W., Beldavs Z.G., Dumyati G., Kainer M.A., Lynfield R., Maloney M., McAllister-Hollod L., Nadle J., et al. Multistate point-prevalence survey of health care-associated infections. N. Engl. J. Med. 2014;370:1198–1208. doi: 10.1056/NEJMoa1306801. - DOI - PMC - PubMed
-
- Kalil A.C., Metersky M.L., Klompas M., Muscedere J., Sweeney D.A., Palmer L.B., Napolitano L.M., O’Grady N.P., Bartlett J.G., Carratalà J., et al. Management of Adults with Hospital-acquired and Ventilator-associated Pneumonia: 2016 Clinical Practice Guidelines by the Infectious Diseases Society of America and the American Thoracic Society. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016;63:61–111. doi: 10.1093/cid/ciw353. - DOI - PMC - PubMed
-
- Torres A., Niederman M.S., Chastre J., Ewig S., Fernandez-Vandellos P., Hanberger H., Kollef M., Li Bassi G., Luna C.M., Martin-Loeches I., et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: Guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociación Latinoamericana del Tórax (ALAT) Eur. Respir. J. 2017;50 doi: 10.1183/13993003.00582-2017. - DOI - PubMed
-
- Esperatti M., Ferrer M., Theessen A., Liapikou A., Valencia M., Saucedo L.M., Zavala E., Welte T., Torres A. Nosocomial pneumonia in the intensive care unit acquired by mechanically ventilated versus nonventilated patients. Am. J. Respir. Crit. Care Med. 2010;182:1533–1539. doi: 10.1164/rccm.201001-0094OC. - DOI - PubMed
