

Immune precision medicine for cancer: a novel insight based on the efficiency of immune effector cells
- PMID: 31200766
- PMCID: PMC6567551
- DOI: 10.1186/s40880-019-0379-3
Immune precision medicine for cancer: a novel insight based on the efficiency of immune effector cells
Abstract
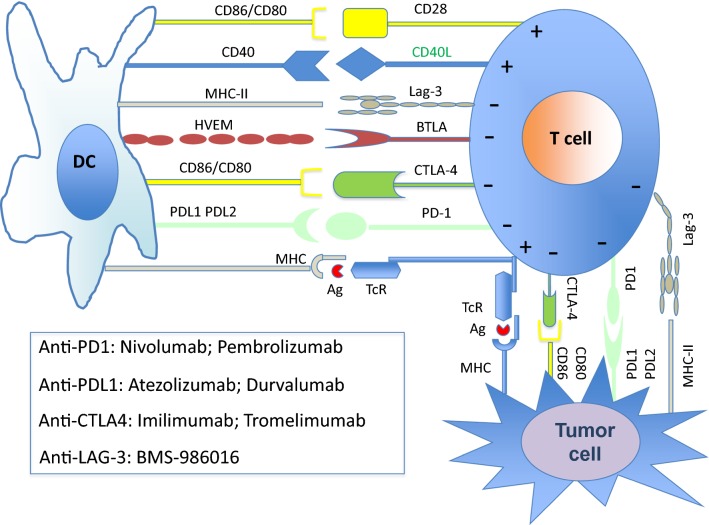
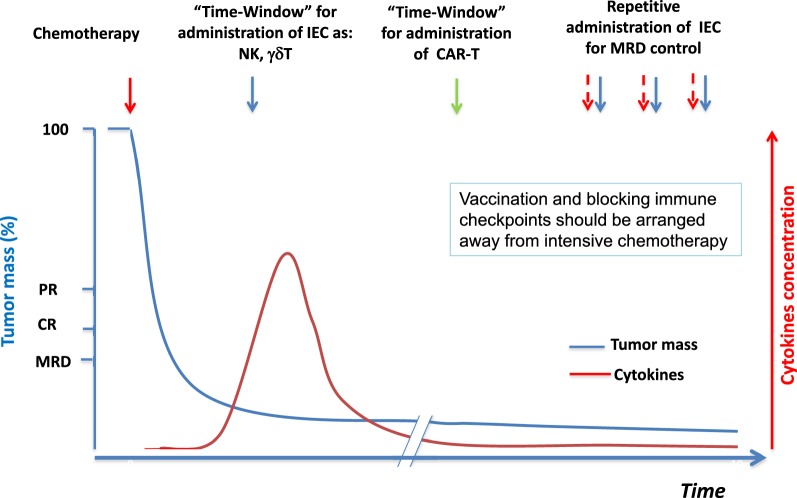
Cancer cell growth is associated with immune surveillance failure. Nowadays, restoring the desired immune response against cancer cells remains a major therapeutic strategy. Due to the recent advances in biological knowledge, efficient therapeutic tools have been developed to support the best bio-clinical approaches for immune precision therapy. One of the most important successes in immune therapy is represented by the applicational use of monoclonal antibodies, particularly the use of rituximab for B-cell lymphoproliferative disorders. More recently, other monoclonal antibodies have been developed, to inhibit immune checkpoints within the tumor microenvironment that limit immune suppression, or to enhance some immune functions with immune adjuvants through different targets such as Toll-receptor agonists. The aim is to inhibit cancer proliferation by the diminishing/elimination of cancer residual cells and clinically improving the response duration with no or few adverse effects. This effect is supported by enhancing the number, functions, and activity of the immune effector cells, including the natural killer (NK) lymphocytes, NKT-lymphocytes, γδ T-lymphocytes, cytotoxic T-lymphocytes, directly or indirectly through vaccines particularly with neoantigens, and by lowering the functions of the immune suppressive cells. Beyond these new therapeutics and their personalized usage, new considerations have to be taken into account, such as epigenetic regulation particularly from microbiota, evaluation of transversal functions, particularly cellular metabolism, and consideration to the clinical consequences at the body level. The aim of this review is to discuss some practical aspects of immune therapy, giving to clinicians the concept of immune effector cells balancing between control and tolerance. Immunological precision medicine is a combination of modern biological knowledge and clinical therapeutic decisions in a global vision of the patient.
Keywords: Cancer; Dendritic cells; Immunotherapy; NK lymphocytes; Precision therapy; T-lymphocytes; Vaccination.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- U.S. National Library of Medicine. What is precision medicine? https://ghr.nlm.nih.gov/primer/precisionmedicine/definition. Accessed 16 May 2019.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
