

Impact of MET inhibitors on survival among patients with non-small cell lung cancer harboring MET exon 14 mutations: a retrospective analysis
- PMID: 31200835
- PMCID: PMC8135929
- DOI: 10.1016/j.lungcan.2019.05.011
Impact of MET inhibitors on survival among patients with non-small cell lung cancer harboring MET exon 14 mutations: a retrospective analysis
Abstract
Objectives: Although dramatic responses to MET inhibitors have been reported in patients with MET exon 14 (METex14) mutant non-small cell lung cancer (NSCLC), the impact of these treatments on overall survival in this population is unknown.
Methods: We conducted a multicenter retrospective analysis of patients with METex14 NSCLC to determine if treatment with MET inhibitors impacts median overall survival (mOS). Event-time distributions were estimated using the Kaplan-Meier method and compared with the log-rank test. Multivariable Cox models were fitted to estimate hazard ratios.
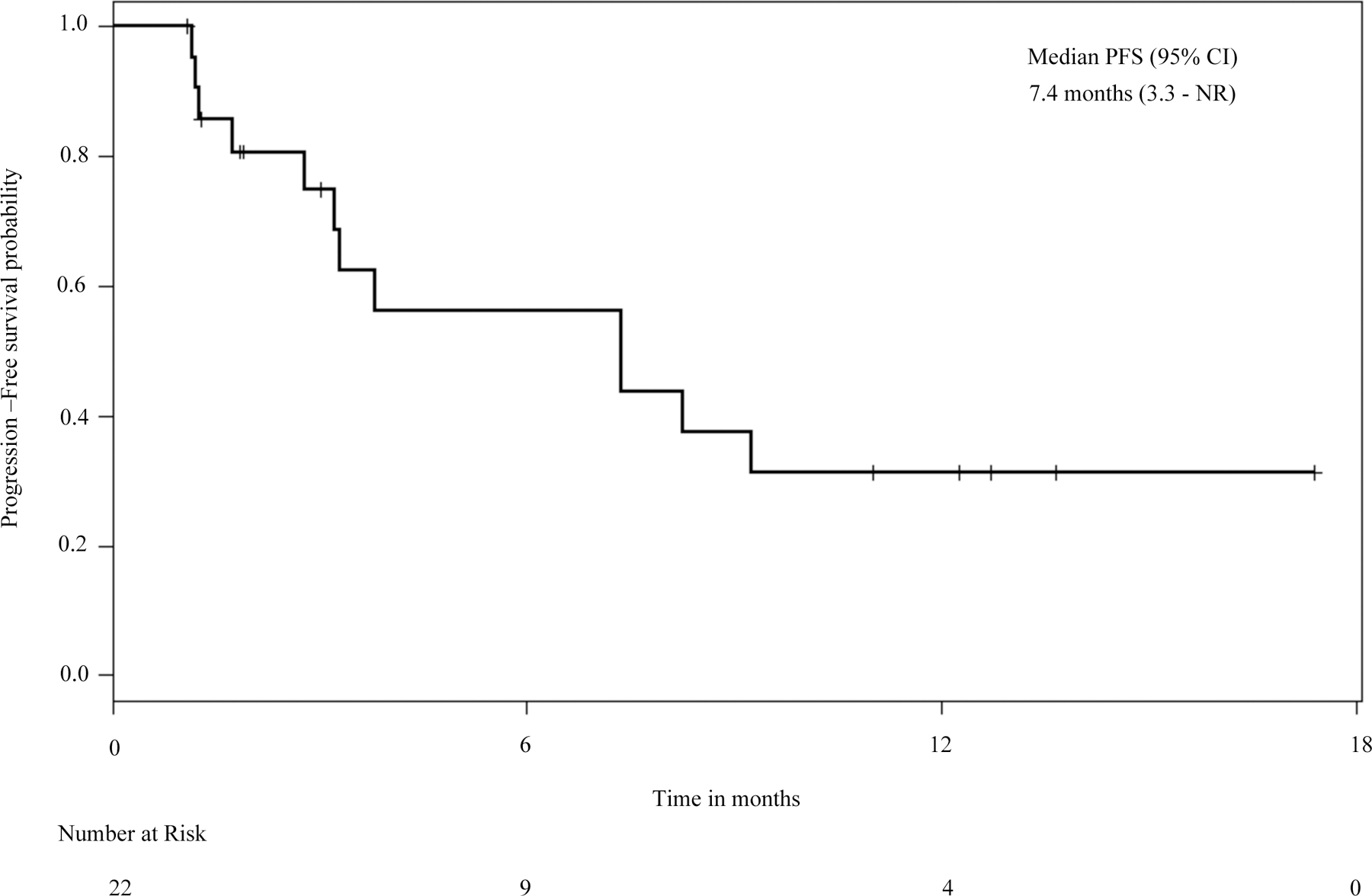
Results: We identified 148 patients with METex14 NSCLC; the median age was 72; 57% were women and 39% were never smokers. Of the 34 metastatic patients who never received a MET inhibitor, the mOS was 8.1 months; those in this group with concurrent MET amplification had a trend toward worse survival compared to cancers without MET amplification (5.2 months vs 10.5 months, P = 0.06). Of the 27 metastatic patients who received at least one MET inhibitor the mOS was 24.6 months. A model adjusting for receipt of a MET inhibitor as first- or second-line therapy as a time-dependent covariate demonstrated that treatment with a MET inhibitor was associated with a significant prolongation in survival (HR 0.11, 95% CI 0.01-0.92, P = 0.04) compared to patients who did not receive any MET inhibitor. Among 22 patients treated with crizotinib, the median progression-free survival was 7.4 months.
Discussion: For patients with METex14 NSCLC, treatment with a MET inhibitor is associated with an improvement in overall survival.
Keywords: MET exon 14; NSCLC; Overall survival; TKI.
Copyright © 2019 Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflict of interest Statement
Dr. Awad reports personal fees from AbbVie, Ariad, Clovis, Bristol-Myers Squibb, Nektar, AstraZeneca, Genentech/Roche, Boehringer Ingelheim, Merck, outside the submitted work. Dr. Dahlberg reports personal fees from AstraZeneca, outside the submitted work. Dr. Drilon reports honoraria from Ignyta, LOXO Oncology, Roche, Astra Zeneca, Ariad, and from TP Therapeutics, outside the submitted work. Noonan is employed by Merck. Dr. Ou reports personal fees from Pfizer, Novartis, and Ignyta, outside the submitted work. Dr. Costa reports personal fees from Pfizer, Ariad, and Boehringer Ingelheim, outside the submitted work. Dr. Gadgeel reports personal fees from Novartis and Pfizer, outside the submitted work. Dr. Steuer reports personal fees from EMD Serono, outside the submitted work. Dr. Forde has received research funding from Novartis and served as consultant to Novartis. Dr. Janne reports personal fees from Pfizer, during the conduct of the study; grants and personal fees from AstraZeneca; personal fees from Boehringher Ingelheim, Roche/Genetech, Ariad Pharmaceuticals, Ignyta, LOXO Oncology, Chugai Pharmaceuticals, Merrimack Pharmaceuticals, grants and personal fees from Eli Lilly and company, grants from Daiichi Sankyo, grants from PUMA, grants from Astellas, outside the submitted work. Dr. Mok reports grants and personal fees from AstraZeneca, Roche/Genentech, Eli Lilly, BMS, Boehringer Ingelheim, Novartis, MSD, Pfizer, Clovis Oncology, Taiho, and SFJ Pharmaceuticals; personal fees from Merck Serono, Vertex, ACEA Biosciences, geneDecode, Oncogenex, Celgene, Ignyta Inc; grants from Eisai; other from Samomics Ltd. and from Cirina, outside the submitted work. Dr. Sholl reports personal fees from Genentech, personal fees from Research to Practice, outside the submitted work. Dr. Heist reports grants from Novartis, Abbvie, Millenium, Genentech Roche, Incyte, Mirati, Celgene, Debiopharm, other from Boehringer Ingelheim, other from Ariad, outside the submitted work. All remaining authors have declared no conflicts of interest.
Figures


References
-
- Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, Nishiwaki Y, Ohe Y, Yang JJ, Chewaskulyong B, Jiang H, Duffield EL, Watkins CL, Armour AA, Fukuoka M, Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma, The New England journal of medicine 361(10) (2009) 947–57. - PubMed
-
- Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C, Zhang S, Wang J, Zhou S, Ren S, Lu S, Zhang L, Hu C, Hu C, Luo Y, Chen L, Ye M, Huang J, Zhi X, Zhang Y, Xiu Q, Ma J, Zhang L, You C, Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study, Lancet Oncol 12(8) (2011) 735–42. - PubMed
-
- Sequist LV, Yang JC, Yamamoto N, O’Byrne K, Hirsh V, Mok T, Geater SL, Orlov S, Tsai CM, Boyer M, Su WC, Bennouna J, Kato T, Gorbunova V, Lee KH, Shah R, Massey D, Zazulina V, Shahidi M, Schuler M, Phase III study of afatinib or cisplatin plus pemetrexed in patients with metastatic lung adenocarcinoma with EGFR mutations, J Clin Oncol 31(27) (2013) 3327–34. - PubMed
-
- Solomon BJ, Mok T, Kim DW, Wu YL, Nakagawa K, Mekhail T, Felip E, Cappuzzo F, Paolini J, Usari T, Iyer S, Reisman A, Wilner KD, Tursi J, Blackhall F, Investigators P, First-line crizotinib versus chemotherapy in ALK-positive lung cancer, The New England journal of medicine 371(23) (2014) 2167–77. - PubMed
-
- Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R, Pallares C, Sanchez JM, Porta R, Cobo M, Garrido P, Longo F, Moran T, Insa A, De Marinis F, Corre R, Bover I, Illiano A, Dansin E, de Castro J, Milella M, Reguart N, Altavilla G, Jimenez U, Provencio M, Moreno MA, Terrasa J, Munoz-Langa J, Valdivia J, Isla D, Domine M, Molinier O, Mazieres J, Baize N, Garcia-Campelo R, Robinet G, Rodriguez-Abreu D, Lopez-Vivanco G, Gebbia V, Ferrera-Delgado L, Bombaron P, Bernabe R, Bearz A, Artal A, Cortesi E, Rolfo C, Sanchez-Ronco M, Drozdowskyj A, Queralt C, de Aguirre I, Ramirez JL, Sanchez JJ, Molina MA, Taron M, Paz-Ares L, Spanish P-C Lung Cancer Group in collaboration with Groupe Francais de, T. Associazione Italiana Oncologia, Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial, Lancet Oncol 13(3) (2012) 239–46. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
