

Predicted effect of regionalised delivery care on neonatal mortality, utilisation, financial risk, and patient utility in Malawi: an agent-based modelling analysis
- PMID: 31200892
- PMCID: PMC6581692
- DOI: 10.1016/S2214-109X(19)30170-6
Predicted effect of regionalised delivery care on neonatal mortality, utilisation, financial risk, and patient utility in Malawi: an agent-based modelling analysis
Abstract
Background: Health-care regionalisation, in which selected services are concentrated in higher-level facilities, has successfully improved the quality of complex medical care. However, the effectiveness of this strategy in routine maternal care is unknown. Malawi has established a national goal of halving its neonatal mortality by 2030. In this study, we aimed to assess the effect of obstetric service regionalisation in pregnant women and their newborn babies in Malawi.
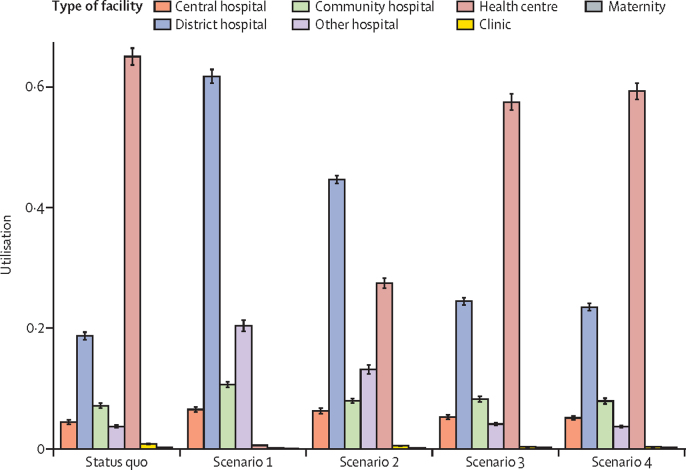
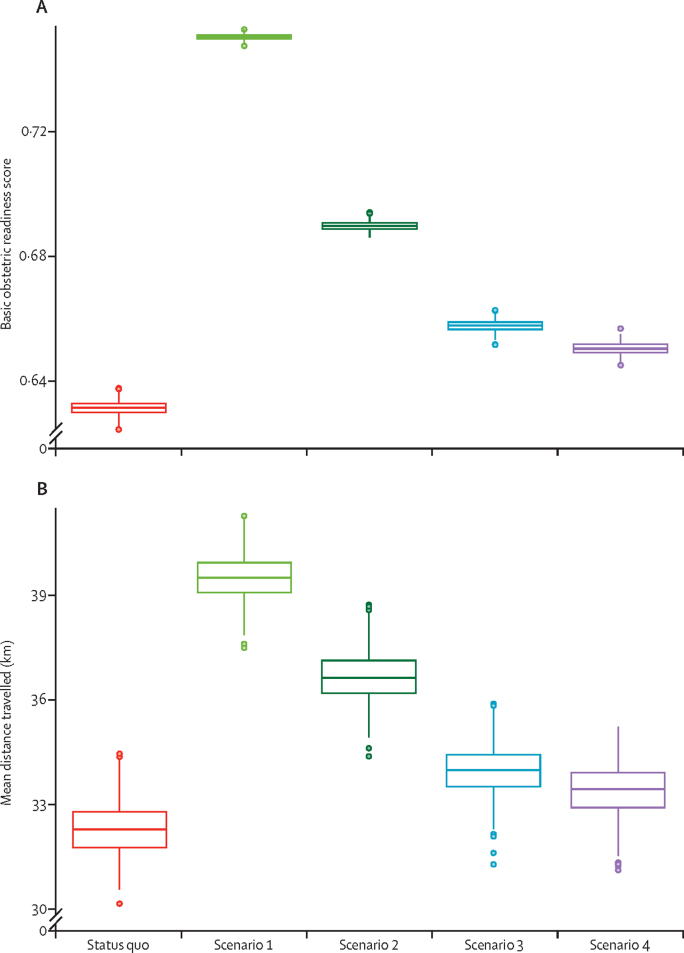
Methods: In this analysis, we assessed regionalisation through the use of an agent-based simulation model. We used a previously estimated utilisation function, incorporating both patient-specific and health-facility-specific characteristics, to inform patient choice. The model was validated against known utilisation patterns in Malawi. Four regionalisation scenarios were compared with the status quo: scenario 1 restricted deliveries to facilities currently capable of providing caesarean sections; scenario 2 had the same restrictions as scenario 1, but with selected facilities upgraded to provide caesarean sections; scenario 3 restricted delivery to facilities that provided five or more basic emergency obstetric and neonatal care services in the preceding 3 months; and scenario 4 had the same restrictions as scenario 3, but with selected facilities upgraded to provide at least five basic emergency obstetric and neonatal care services. We assessed neonatal mortality, utilisation, travel distance, median out-of-pocket expenditure, and proportion of women facing catastrophic expenditure. The effects of upgrading the obstetric readiness of all facilities, of removing all user fees, and of upgrading without restriction were considered in scenario analyses. Heterogeneity and parameter uncertainty were incorporated to create 95% posterior credible intervals (PCIs).
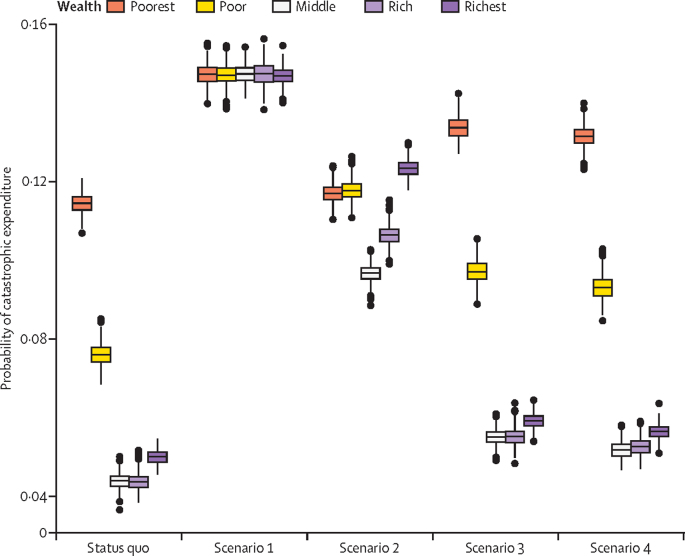
Findings: Scenarios restricting women to give birth in facilities with caesarean section capabilities reduced neonatal mortality by 11·4 deaths per 1000 livebirths (scenario 1; 95% PCI 9·8-13·1) and 11·6 deaths per 1000 livebirths (scenario 2; 10·2-13·1), whereas scenarios restricting women to facilities that provided five or more basic emergency obstetric and neonatal care services did not affect neonatal mortality. Similarly, the caesarean section rate in Malawi, which is 4·6% under the status quo, was predicted to rise significantly in scenario 1 (14·7%, 95% PCI 14·5-14·9; p<0·0001) and scenario 2 (10·4%, 10·2-10·6; p<0·0001), but not in scenarios 3 and 4. Women were required to travel longer distances in scenario 1 (increase of 7·2 km, 95% PCI 4·5-9·9) and in scenario 2 (4·4 km, 1·5-7·2) than in the status quo (p<0·0001). Out-of-pocket costs tripled (p<0·0001; status quo vs scenario 1 and scenario 2), and the risk of catastrophic expenditure significantly increased from a baseline of 6·4% (95% PCI 6·1-6·6) to 14·7% (14·5-14·9) in scenario 1 and 11·3% (11·0-11·5) in scenario 2. This increase was especially pronounced among the poor (p<0·0001; status quo vs scenario 1 and scenario 2).
Interpretation: Policies restricting women to give birth in facilities with caesarean section capabilities is likely to result in significant decreases in neonatal mortality and might allow Malawi to meet its goal of halving its neonatal mortality by 2030. However, this improvement comes at the cost of increased distances to care and worsening financial risks among women.
Funding: Bill & Melinda Gates Foundation, Damon Runyon Cancer Research Foundation.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Potential effect of regionalised care in a low-resource setting.Lancet Glob Health. 2019 Jul;7(7):e825-e826. doi: 10.1016/S2214-109X(19)30235-9. Lancet Glob Health. 2019. PMID: 31200880 No abstract available.
References
-
- Mazalale J, Kambala C, Brenner S. Factors associated with delivery outside a health facility: cross-sectional study in rural Malawi. Trop Med Int Health. 2015;20:617–626. - PMC - PubMed
- Mazalale J, Kambala C, Brenner S, et al. Factors associated with delivery outside a health facility: cross-sectional study in rural Malawi. Trop Med Int Health 2015; 20: 617–26. - PMC - PubMed
-
- Malik AT, Mufarrih SH, Ali A, Noordin S. Does surgeon volume affect the outcome of total knee arthroplasties in a developing country? A retrospective cohort study. Ann Med Surg. 2017;24:38–43. - PMC - PubMed
- Malik AT, Mufarrih SH, Ali A, Noordin S. Does surgeon volume affect the outcome of total knee arthroplasties in a developing country? A retrospective cohort study. Ann Med Surg 2017; 24: 38–43. - PMC - PubMed
-
- Malik AT, Panni UY, Masri BA, Noordin S. The impact of surgeon volume and hospital volume on postoperative mortality and morbidity after hip fractures: a systematic review. Int J Surg. 2018;54:316–327. - PubMed
- Malik AT, Panni UY, Masri BA, Noordin S. The impact of surgeon volume and hospital volume on postoperative mortality and morbidity after hip fractures: a systematic review. Int J Surg 2018; 54: 316–27. - PubMed
-
- Nieman CL, Stewart CM, Eisele DW, Pronovost PJ, Gourin CG. Frailty, hospital volume, and failure to rescue after head and neck cancer surgery. Laryngoscope. 2017;128:1365–1370. - PubMed
- Nieman CL, Stewart CM, Eisele DW, Pronovost PJ, Gourin CG. Frailty, hospital volume, and failure to rescue after head and neck cancer surgery. Laryngoscope 2017; 128: 1365–70. - PubMed
-
- Chapman BC, Paniccia A, Hosokawa PW. Impact of facility type and surgical volume on 10-year survival in patients undergoing hepatic resection for hepatocellular carcinoma. J Am Coll Surg. 2017;224:362–372. - PubMed
- Chapman BC, Paniccia A, Hosokawa PW, et al. Impact of facility type and surgical volume on 10-year survival in patients undergoing hepatic resection for hepatocellular carcinoma. J Am Coll Surg 2017; 224: 362–72. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
