

Distinct nasal airway bacterial microbiotas differentially relate to exacerbation in pediatric patients with asthma
- PMID: 31201890
- PMCID: PMC6842413
- DOI: 10.1016/j.jaci.2019.05.035
Distinct nasal airway bacterial microbiotas differentially relate to exacerbation in pediatric patients with asthma
Abstract
Background: In infants, distinct nasopharyngeal bacterial microbiotas differentially associate with the incidence and severity of acute respiratory tract infection and childhood asthma development.
Objective: We hypothesized that distinct nasal airway microbiota structures also exist in children with asthma and relate to clinical outcomes.
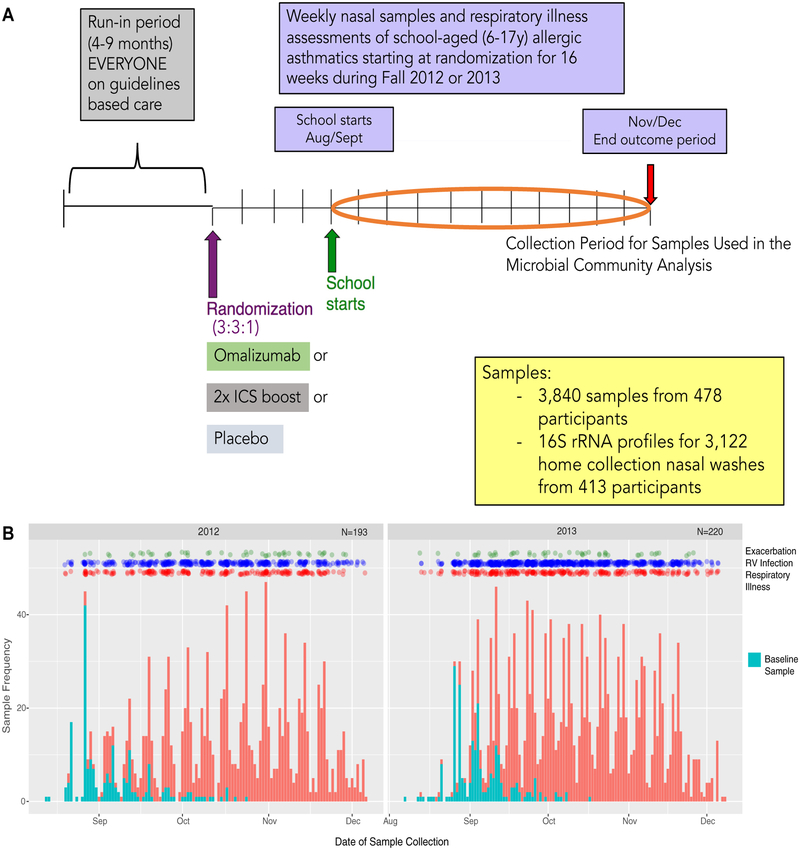
Methods: Nasal secretion samples (n = 3122) collected after randomization during the fall season from children with asthma (6-17 years, n = 413) enrolled in a trial of omalizumab (anti-IgE) underwent 16S rRNA profiling. Statistical analyses with exacerbation as the primary outcome and rhinovirus infection and respiratory illnesses as secondary outcomes were performed. Using A549 epithelial cells, we assessed nasal isolates of Moraxella, Staphylococcus, and Corynebacterium species for their capacity to induce epithelial damage and inflammatory responses.
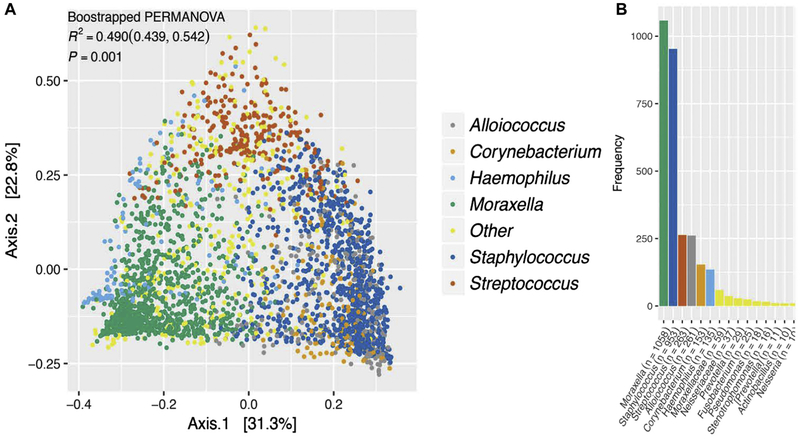
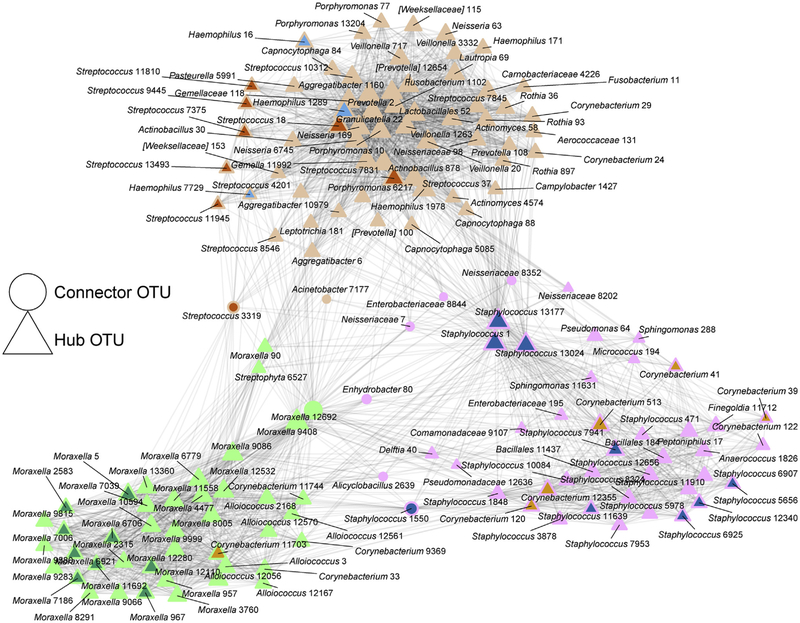
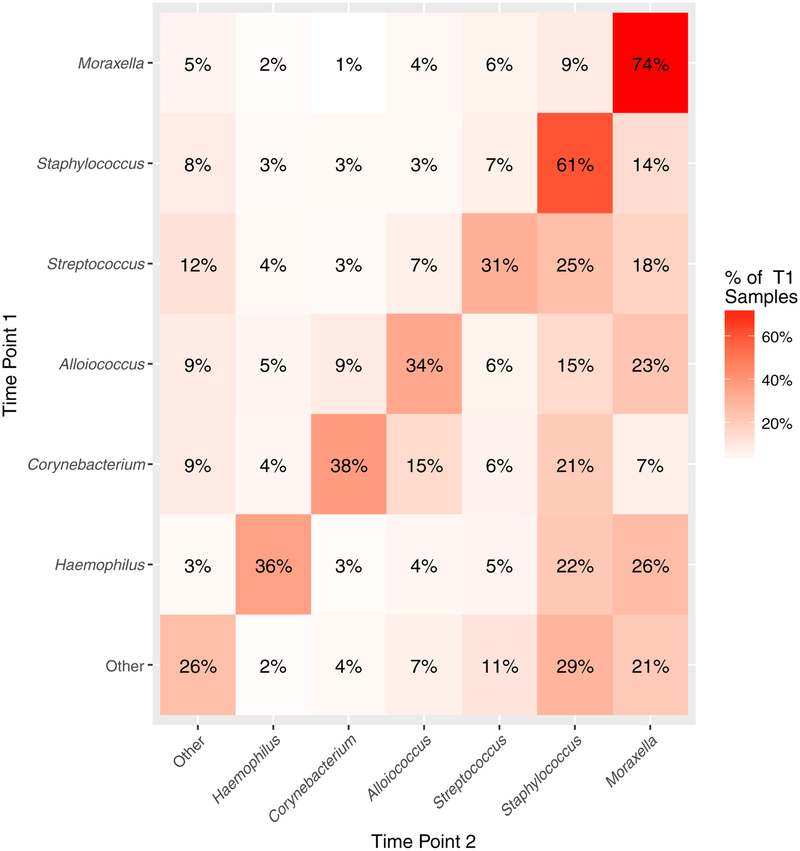
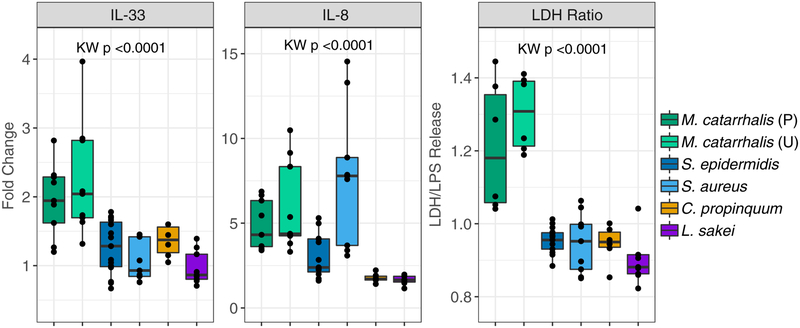
Results: Six nasal airway microbiota assemblages, each dominated by Moraxella, Staphylococcus, Corynebacterium, Streptococcus, Alloiococcus, or Haemophilus species, were observed. Moraxella and Staphylococcus species-dominated microbiotas were most frequently detected and exhibited temporal stability. Nasal microbiotas dominated by Moraxella species were associated with increased exacerbation risk and eosinophil activation. Staphylococcus or Corynebacterium species-dominated microbiotas were associated with reduced respiratory illness and exacerbation events, whereas Streptococcus species-dominated assemblages increased the risk of rhinovirus infection. Nasal microbiota composition remained relatively stable despite viral infection or exacerbation; only a few taxa belonging to the dominant genera exhibited relative abundance fluctuations during these events. In vitro, Moraxella catarrhalis induced significantly greater epithelial damage and inflammatory cytokine expression (IL-33 and IL-8) compared with other dominant nasal bacterial isolates tested.
Conclusion: Distinct nasal airway microbiotas of children with asthma relate to the likelihood of exacerbation, rhinovirus infection, and respiratory illnesses during the fall season.
Keywords: 16S rRNA; Microbiota; Moraxella species; Staphylococcus species; airway; asthma; exacerbation; rhinovirus.
Copyright © 2019. Published by Elsevier Inc.
Conflict of interest statement
Disclosure of potential conflict of interest: All authors, with the exception of A. Togias, report grants from the National Institutes of Health (NIH) during the conduct of study. R. Valladares reports personal fees for employment with Siolta Therapeutics outside the submitted work. H. T. Tran reports personal fees from GlaxoSmithKline outside the submitted work. J. Pongracic reports provision of study drug for other asthma and allergy studies from GlaxoSmithKline, Boehringer Ingelheim, and Genentech/Novartis outside the submitted work. C. M. Kercsmar reports personal fees from GlaxoSmithKline for service on a DSMB and royalties from UpToDate outside the submitted work. M. Gill reports honoraria and support for travel from the American Academy of Allergy, Asthma & Immunology (AAAAI), as well as payment for lectures from the American Academy of Pediatrics outside the submitted work. A.H. Liu reports personal fees from Merck Sharp & Dohme and Phadia Thermo-Fisher and membership on a Data Monitoring Committee for GlaxoSmithKline outside the submitted work. M. Kattan reports personal feed from Novartis Pharma and Regeneron for service on advisory boards outside the submitted work. S. J. Teach reports grants from Patient-Centered Outcomes Research Institute (PCORI), EJF, and the NIH/National Heart, Lung, and Blood Institute (NHLBI) outside the submitted work and personal fees from UpToDate outside the submitted work. H. A. Boushey serves as a compensated member of a Scientific Advisory Committee for Siolta Therapeutics. J. E. Gern reports personal fees from PREP Biopharm, Regeneron, Meissa Vaccines, MedImmune, and Ena Pharmaceuticals, as well as stock options from Meissa Vaccines outside the submitted work and has a patent “Methods of Propagating Rhinovirus C in Previously Unsusceptible Cell Lines” issued and a patent “Adapted Rhinovirus C” pending outside the submitted work. D. J. Jackson reports personal fees from Novartis, Boehringer Ingelheim, Pfizer, Commense, and Sanofi/Genzyme outside the submitted work, as well as grants from GlaxoSmithKline and the NIH/NHLBI. S.V. Lynch reports grants from the NIH/National Institute of Allergy and Infectious Diseases (NIAID), NIH/National Institute on Drug Abuse (NIDA), NIH/Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD), NIH/Office of the Director, and the Crohn’s and Colitis Foundation of America; reports personal fees from Siolta Therapeutics outside the submitted work; has a patent “Reductive prodrug cancer chemotherapy (Stan449-PRV)” issued, a patent “Combination antibiotic and antibody therapy for the treatment of
Figures
References
-
- Bisgaard H, Hermansen MN, Buchvald F, Loland L, Halkjaer LB, Bønnelykke K, et al. Childhood asthma after bacterial colonization of the airway in neonates. N Engl J Med 2007;357:1487–95. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UM1 AI109565/AI/NIAID NIH HHS/United States
- UL1 TR000150/TR/NCATS NIH HHS/United States
- UL1 TR001105/TR/NCATS NIH HHS/United States
- UL1 TR000075/TR/NCATS NIH HHS/United States
- UL1 RR025780/RR/NCRR NIH HHS/United States
- UM2 AI117870/AI/NIAID NIH HHS/United States
- UH3 OD023282/OD/NIH HHS/United States
- UL1 TR001082/TR/NCATS NIH HHS/United States
- HHSN272200900052C/AI/NIAID NIH HHS/United States
- HHSN272201000052I/AI/NIAID NIH HHS/United States
- UL1 TR000154/TR/NCATS NIH HHS/United States
- R01 AI098077/AI/NIAID NIH HHS/United States
- UL1 TR000451/TR/NCATS NIH HHS/United States
- UM1 AI114271/AI/NIAID NIH HHS/United States
- T32 GM008568/GM/NIGMS NIH HHS/United States
- UL1 TR001425/TR/NCATS NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- UL1 TR000077/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
