

Metastasis as a systemic disease: molecular insights and clinical implications
- PMID: 31202687
- PMCID: PMC6692219
- DOI: 10.1016/j.bbcan.2019.06.002
Metastasis as a systemic disease: molecular insights and clinical implications
Abstract
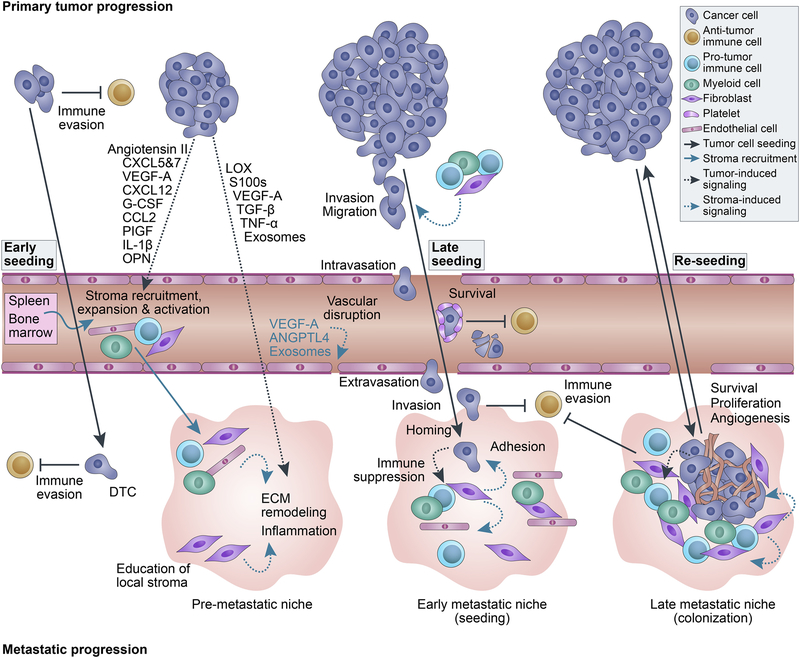
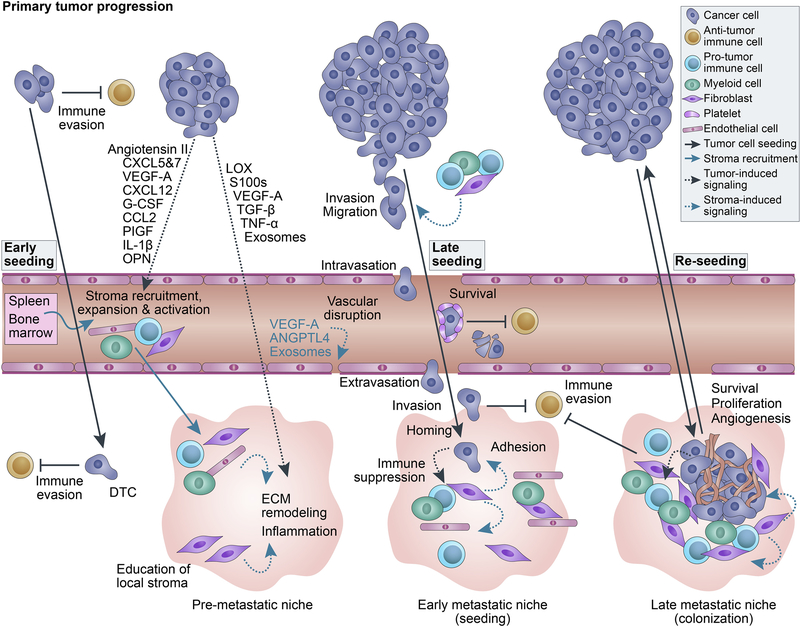
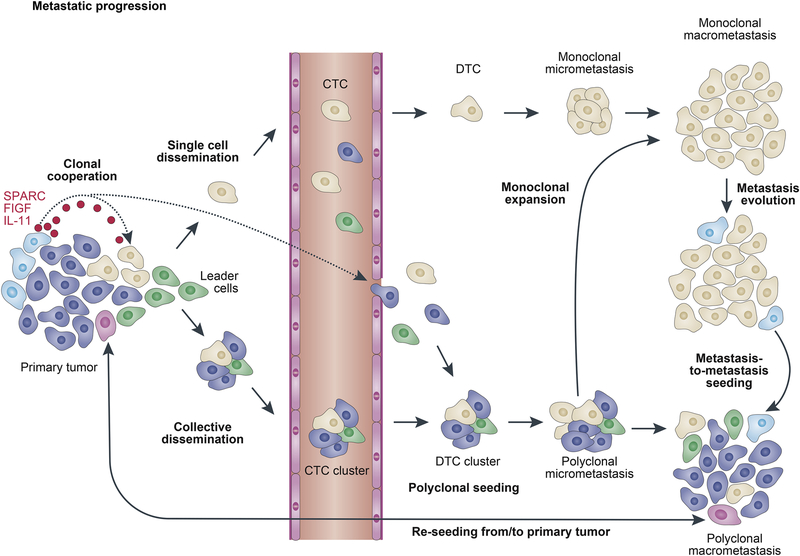
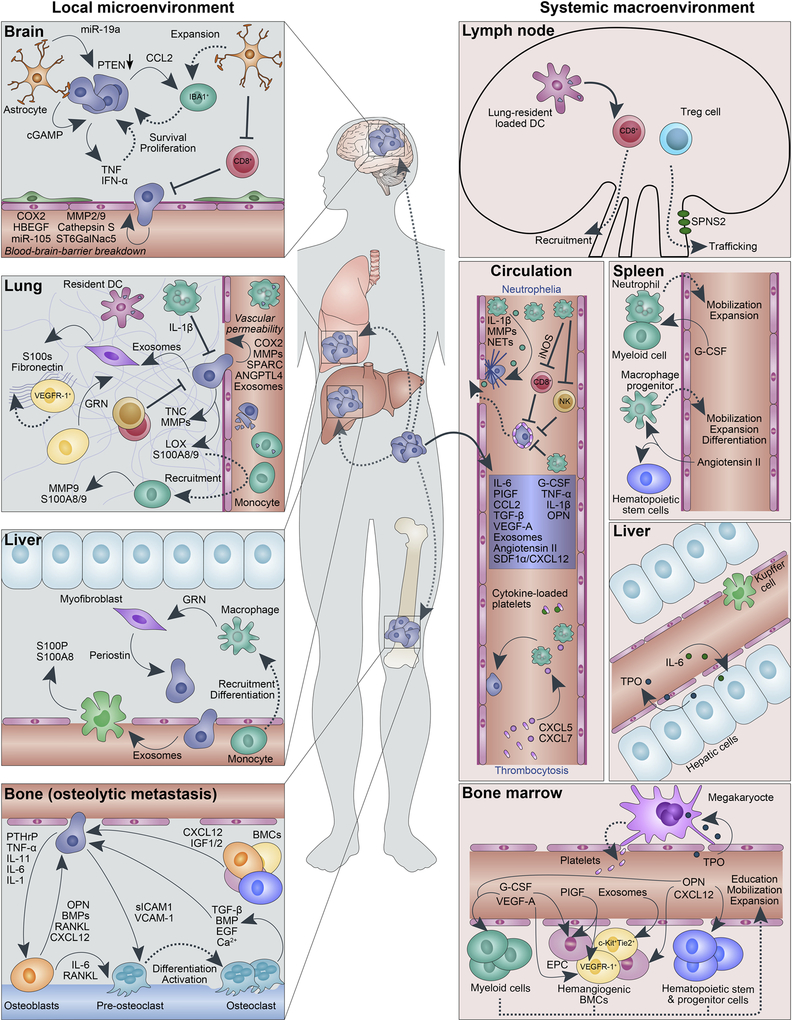
Metastasis is a complex systemic disease that develops as a result of interactions between tumor cells and their local and distant microenvironments. Local and systemic immune-related changes play especially critical roles in limiting or enabling the development of metastatic disease. Although anti-tumor immune responses likely eliminate most early primary and metastatic lesions, factors secreted by cancer or stromal cells in the primary tumor can mobilize and activate cells in distant organs in a way that promotes the outgrowth of disseminated cancer cells into macrometastatic lesions. Therefore, the prevention, detection, and effective treatment of metastatic disease require a deeper understanding of the systemic effects of primary tumors as well as predisposing hereditary and acquired host factors including chronic inflammatory conditions. The success of immunotherapy in a subset of cancer patients is an example of how modulating the microenvironment and tumor-immune cell interactions can be exploited for the effective eradiation of even advanced-stage tumors. Here, we highlight emerging insights and clinical implications of cancer as a systemic disease.
Keywords: Host factors; Metastasis; Systemic effects.
Copyright © 2019 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
COMPETING FINANCIAL INTERESTS
K. Polyak serves on the scientific advisory boards of Mitra Biotech and Acrivon THerapeutics.
Figures
References
-
- Chaffer CL, Weinberg RA, A Perspective on Cancer Cell Metastasis, Science 331(6024) (2011) 1559–1564. - PubMed
-
- Siegel RL, Miller KD, Jemal A, Cancer statistics, 2018, CA: A Cancer Journal for Clinicians 68(1) (2018) 7–30. - PubMed
-
- Celiá-Terrassa T, Kang Y, Metastatic niche functions and therapeutic opportunities, Nature Cell Biology 20(8) (2018) 868–877. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
