

Diastolic Dysfunction and Heart Failure With Preserved Ejection Fraction: Understanding Mechanisms by Using Noninvasive Methods
- PMID: 31202759
- PMCID: PMC6899218
- DOI: 10.1016/j.jcmg.2018.12.034
Diastolic Dysfunction and Heart Failure With Preserved Ejection Fraction: Understanding Mechanisms by Using Noninvasive Methods
Abstract
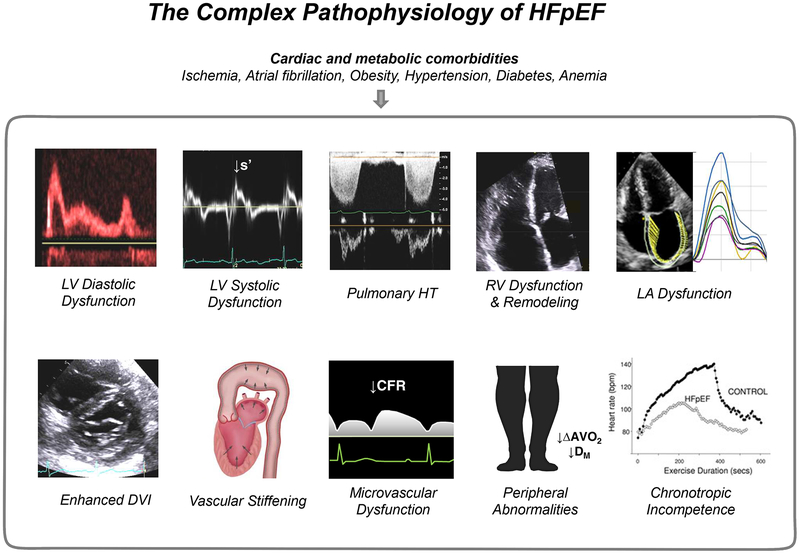
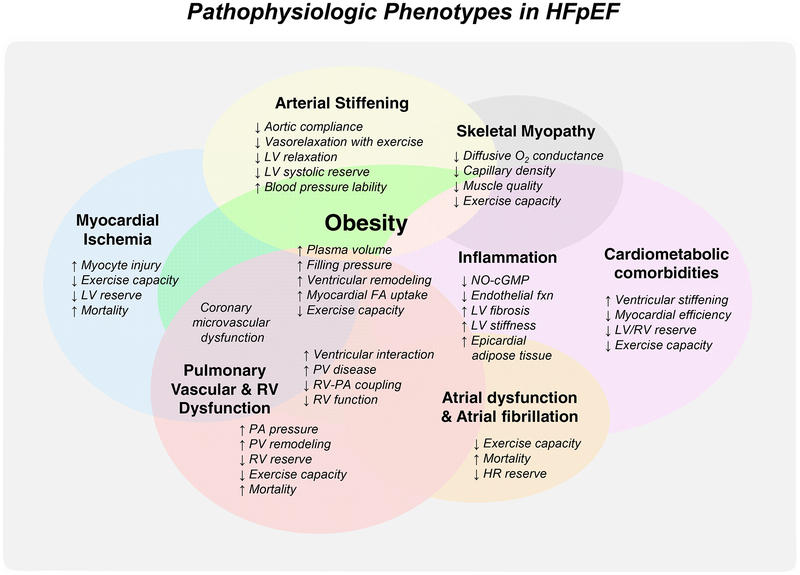
Research in the last decade has substantially advanced our understanding of the pathophysiology of heart failure with preserved ejection fraction (HFpEF). However, treatment options remain limited as clinical trials have largely failed to identify effective therapies. Part of this failure may be related to mechanistic heterogeneity. It is speculated that categorizing HFpEF patients based upon underlying pathophysiological phenotypes may represent the key next step in delivering the right therapies to the right patients. Echocardiography may provide valuable insight into both the pathophysiology and underlying phenotypes in HFpEF. Echocardiography also plays a key role in the evaluation of patients with unexplained dyspnea, where HFpEF is suspected but the diagnosis remains unknown. The combination of the E/e' ratio and right ventricular systolic pressure has recently been shown to add independent value to the diagnostic evaluation of patients suspected of having HFpEF. Finally, echocardiography enables identification of the different causes that mimic HFpEF but are treated differently, such as valvular heart disease, pericardial constriction, and high-output heart failure or infiltrative myopathies such as cardiac amyloid. This review summarizes the current understanding of the pathophysiology and phenotyping of HFpEF with particular attention to the role of echocardiography in this context.
Keywords: diagnosis; diastolic function; echocardiography; filling pressure; heart failure; noninvasive.
Copyright © 2020 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Diastolic Stress Testing: Have You Considered Isometric Handgrip Echocardiography?JACC Cardiovasc Imaging. 2019 Oct;12(10):2095-2097. doi: 10.1016/j.jcmg.2019.07.023. JACC Cardiovasc Imaging. 2019. PMID: 31601382 Free PMC article. No abstract available.
-
The Authors Reply.JACC Cardiovasc Imaging. 2019 Oct;12(10):2098-2099. doi: 10.1016/j.jcmg.2019.07.024. JACC Cardiovasc Imaging. 2019. PMID: 31601384 No abstract available.
References
-
- Borlaug BA. The pathophysiology of heart failure with preserved ejection fraction. Nat Rev Cardiol. 2014;11:507–15. - PubMed
-
- Nagueh SF, Smiseth OA, Appleton CP, et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr. 2016;29:277–314. - PubMed
-
- Brutsaert DL, Sys SU, Gillebert TC. Diastolic failure: pathophysiology and therapeutic implications. J Am Coll Cardiol. 1993;22:318–25. - PubMed
-
- Gaasch WH, Zile MR. Left ventricular diastolic dysfunction and diastolic heart failure. Annu Rev Med. 2004;55:373–94. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
