

Comparison of Magnetic Resonance Imaging-stratified Clinical Pathways and Systematic Transrectal Ultrasound-guided Biopsy Pathway for the Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-analysis of Randomized Controlled Trials
- PMID: 31204311
- PMCID: PMC7406122
- DOI: 10.1016/j.euo.2019.05.004
Comparison of Magnetic Resonance Imaging-stratified Clinical Pathways and Systematic Transrectal Ultrasound-guided Biopsy Pathway for the Detection of Clinically Significant Prostate Cancer: A Systematic Review and Meta-analysis of Randomized Controlled Trials
Abstract
Context: Recent studies suggested that magnetic resonance imaging (MRI) followed by targeted biopsy ("MRI-stratified pathway") detects more clinically significant prostate cancers (csPCa) than the systematic transrectal ultrasound-guided prostate biopsy (TRUS-Bx) pathway, but controversy persists. Several randomized clinical trials (RCTs) were recently published, enabling generation of higher-level evidence to evaluate this hypothesis.
Objective: To perform a systematic review and meta-analysis of RCTs comparing the detection rates of csPCa in the MRI-stratified pathway and the systematic TRUS-Bx pathway in patients with a suspicion of prostate cancer (PCa).
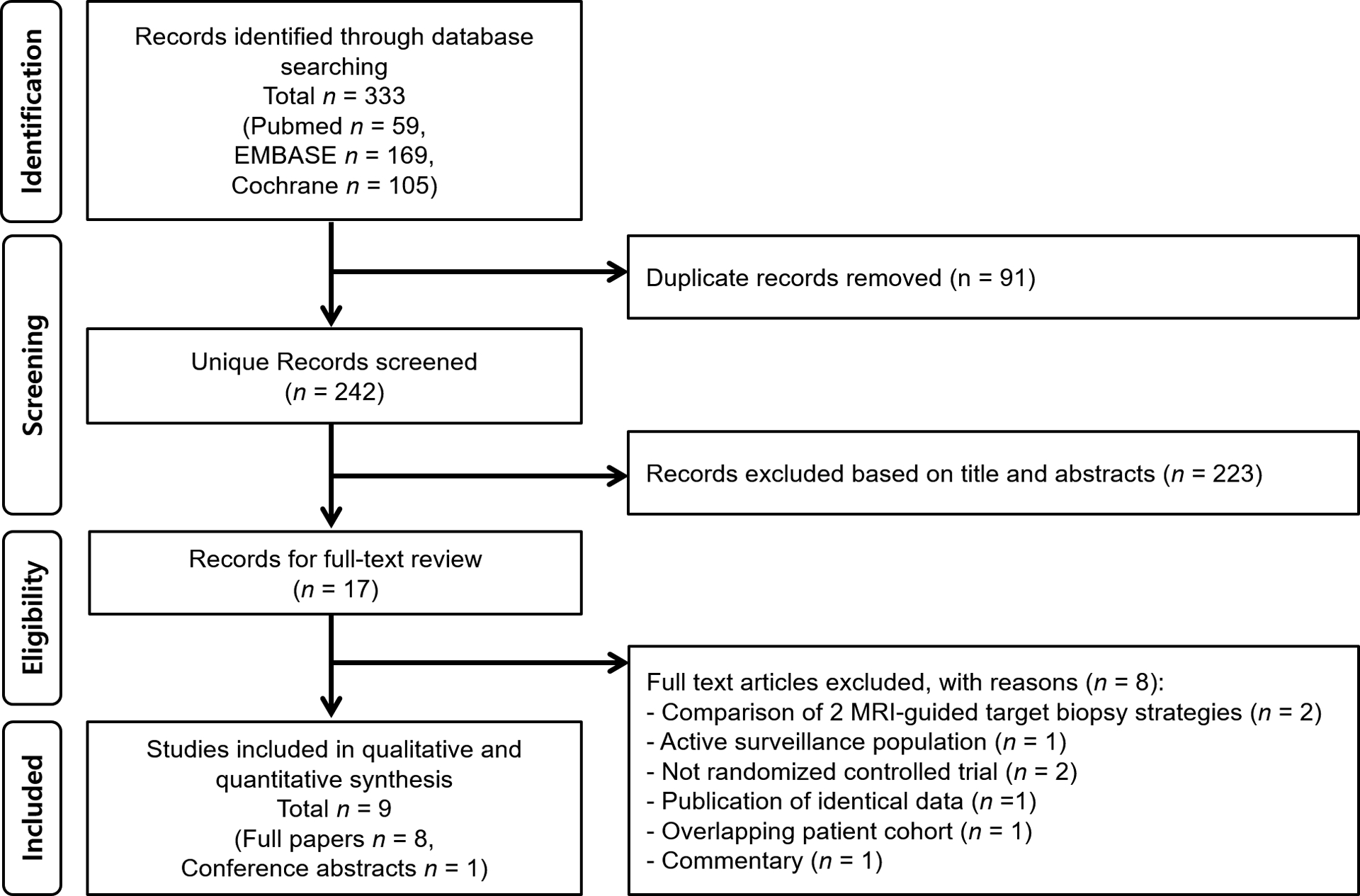
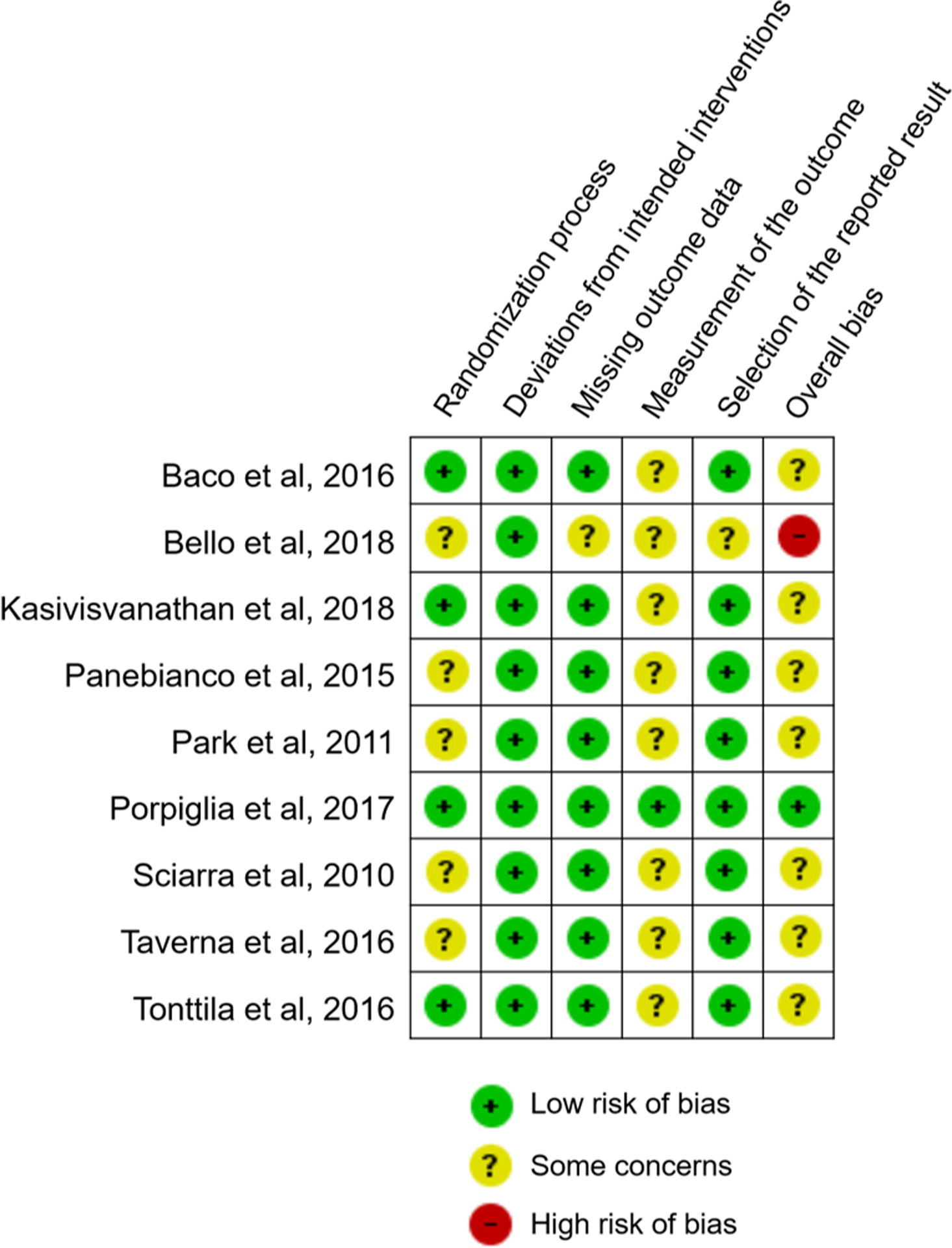
Evidence acquisition: PubMed, EMBASE, and Cochrane databases were searched up to March 18, 2019. RCTs reporting csPCa detection rates of both pathways in patients with a clinical suspicion of prostate cancer were included. Relative csPCa detection rates of the MRI-stratified pathway were pooled using random-effect model. Study quality was assessed using the Cochrane risk of bias tool for randomized trials. A comparison of detection rates of clinically insignificant PCa (cisPCa) and any PCa was also performed.
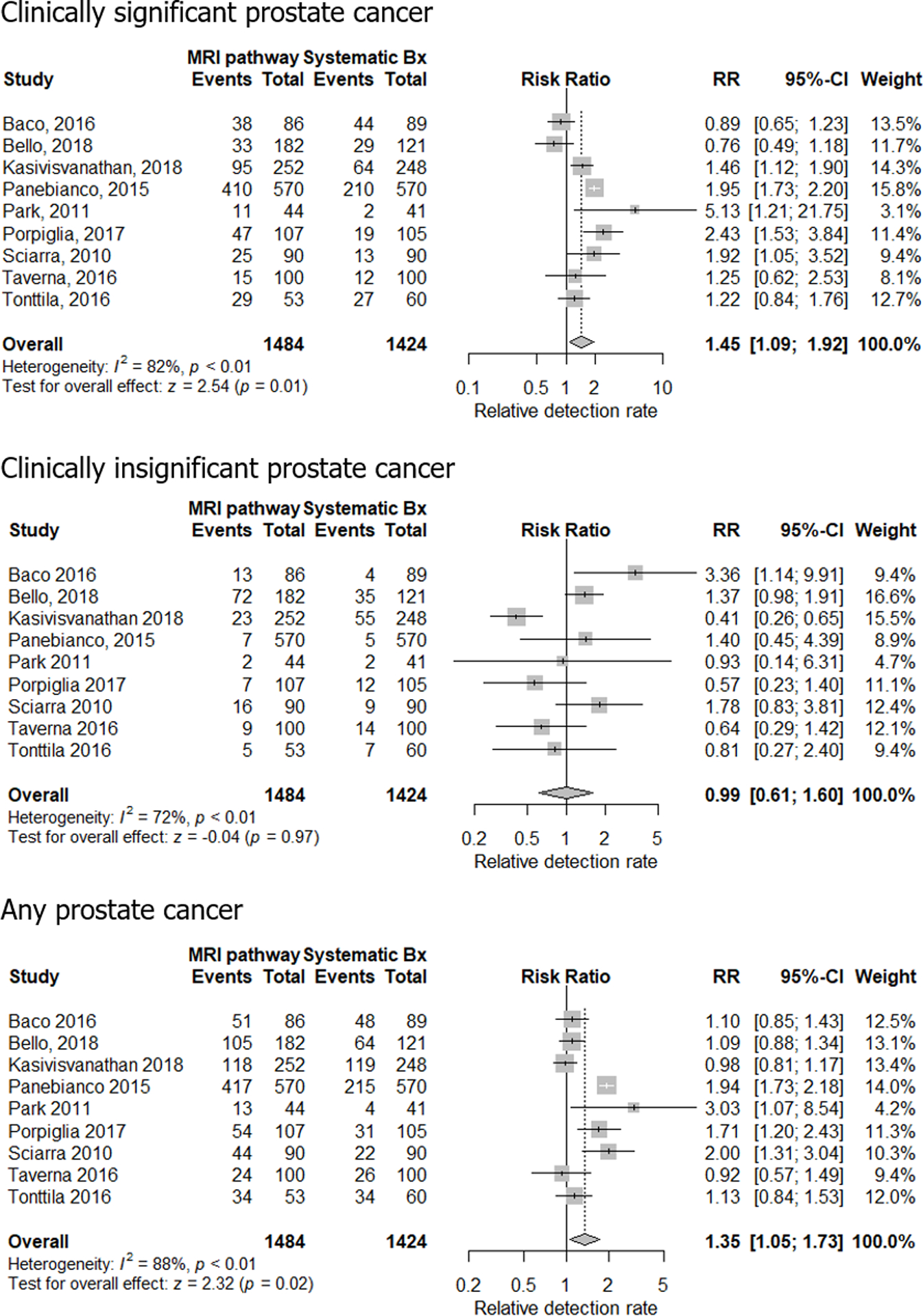
Evidence synthesis: Nine RCTs (2908 patients) were included. The MRI-stratified pathway detected more csPCa than the TRUS-Bx pathway (relative detection rate 1.45 [95% confidence interval {CI} 1.09-1.92] for all patients, and 1.42 [95% CI 1.02-1.97] and 1.60 [95% CI 1.01-2.54] for biopsy-naïve and prior negative biopsy patients, respectively). Detection rates were not significantly different between pathways for cisPCa (0.89 [95% CI 0.49-1.62]), but higher in the MRI-stratified pathway for the detection of any PCa (1.39 [95% CI 1.05-1.84]).
Conclusions: The MRI-stratified pathway detected more csPCa than the systematic TRUS-guided biopsy pathway in men with a clinical suspicion of PCa, for both biopsy-naïve patients and those with prior negative biopsy. The detection rate of any PCa was higher in the MRI-stratified pathway, but not significantly different from that of cisPCa.
Patient summary: Our meta-analysis of clinical trials shows that the magnetic resonance imaging-stratified pathway detects more clinically significant prostate cancers than the transrectal ultrasound-guided prostate biopsy pathway in men with a suspicion of prostate cancer.
Keywords: Biopsy; Magnetic resonance imaging; Meta-analysis; Prostate cancer; Systematic review; Targeted biopsy.
Copyright © 2019 European Association of Urology. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Eichler K, Hempel S, Wilby J, Myers L, Bachmann LM, Kleijnen J. Diagnostic value of systematic biopsy methods in the investigation of prostate cancer: a systematic review. J Urol 2006;175:1605–12. - PubMed
-
- Geiger-Gritsch S, Oberaigner W, Muhlberger N, et al. Patient-reported urinary incontinence and erectile dysfunction following radical prostatectomy: results from the European Prostate Centre Innsbruck. Urol Int 2015;94:419–27. - PubMed
-
- Vargas HA, Hotker AM, Goldman DA, et al. Updated Prostate Imaging Reporting and Data System (PIRADS v2) recommendations for the detection of clinically significant prostate cancer using multiparametric MRI: critical evaluation using whole-mount pathology as standard of reference. Eur Radiol 2016;26:1606–12. - PMC - PubMed
-
- Ahmed HU, El-Shater Bosaily A, Brown LC, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study. Lancet 2017;389:815–22. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
